

Subacromial impingement (SAI) is a medical condition characterized by the rubbing or pinching of the tendons of the rotator cuff (a group of muscles and tendons surrounding the shoulder) beneath the acromion, a bony prominence of the shoulder blade.
Synonym
- Subacromial Impingement Syndrome
- Neer Subacromial Impingement
- CSA (Subacromial Impingement)
- Impingement Shoulder
- Shoulder Abutment Syndrome
- Impingement Syndrome subacromial
Introduction
Understanding Shoulder Impingement Syndrome: A Comprehensive Overview
Shoulder impingement syndrome is a common condition that affects the shoulder joint, causing pain and restricting movement. Often resulting from repetitive overhead activities or poor posture, this condition impacts individuals ranging from athletes to desk workers. The shoulder, being one of the most mobile joints in the body, is particularly vulnerable to injuries and syndromes like impingement due to its intricate structure and constant use in daily activities.
This syndrome occurs when the tendons or bursae in the shoulder become compressed, inflamed, or irritated as they pass through the narrow space beneath the acromion (part of the shoulder blade). This compression can lead to pain, weakness, and reduced range of motion, making simple activities like reaching overhead, lifting objects, or even sleeping on the affected side uncomfortable.
While shoulder impingement syndrome can affect anyone, certain groups are more predisposed. Athletes involved in sports requiring repetitive overhead motions, such as swimming, baseball, or tennis, are at a higher risk. Additionally, individuals with occupations or hobbies involving prolonged overhead movements or improper posture may also develop the condition over time. Age is another contributing factor, as the tendons in the shoulder naturally degenerate with time, making them more susceptible to injury.
The symptoms of shoulder impingement often begin subtly but can escalate if left untreated. These include pain during movement, difficulty lifting the arm, a sensation of weakness, and even discomfort at rest. Early diagnosis and treatment are crucial to prevent the condition from worsening and to maintain shoulder function.
Fortunately, shoulder impingement syndrome is highly treatable. Non-surgical approaches, such as physical therapy, anti-inflammatory medications, and lifestyle modifications, are often sufficient to alleviate symptoms and restore function. These interventions aim to reduce inflammation, strengthen the shoulder muscles, and improve posture, minimizing the likelihood of recurrence. In severe cases, when conservative treatments fail, surgical options such as subacromial decompression may be considered to relieve the pressure on the affected tissues.
In this article, we delve into the causes, symptoms, and treatment options for shoulder impingement syndrome. Whether you are experiencing symptoms or seeking preventative strategies, understanding this condition is the first step toward effective management and maintaining a healthy, pain-free shoulder.
Anatomy of the Shoulder: Key Structures and Their Roles
The shoulder is one of the most complex and mobile joints in the human body, designed to provide a wide range of motion while maintaining stability. Its intricate anatomy is essential for everyday activities, from lifting and throwing to reaching and pushing. Understanding the shoulder’s key structures and their roles is crucial to grasp how conditions like shoulder impingement syndrome develop.
Key Structures Involved
The shoulder is composed of three primary bones and a network of muscles, tendons, and ligaments that work together harmoniously:
- Bones:
- Humerus: The upper arm bone forms the ball of the ball-and-socket joint in the shoulder.
- Scapula (Shoulder Blade): This flat, triangular bone includes the acromion and provides a stable base for shoulder muscles.
- Clavicle (Collarbone): Connects the shoulder to the chest, providing structural support and stability.
- Joints:
- Glenohumeral Joint: The primary ball-and-socket joint of the shoulder, allowing rotational and forward/backward movements.
- Acromioclavicular Joint: Located between the acromion and the clavicle, crucial for overhead movements.
- Sternoclavicular Joint: Connects the clavicle to the sternum, aiding in overall shoulder stability.
- Muscles:
- The deltoid and pectoralis major provide power for large shoulder movements.
- The rotator cuff muscles, comprising the supraspinatus, infraspinatus, teres minor, and subscapularis, stabilize the humeral head in the shoulder socket during motion.
- Tendons and Ligaments:
- Rotator Cuff Tendons: These attach the rotator cuff muscles to the bones, enabling movement and stability.
- Coracoacromial Ligament: Connects the acromion to the coracoid process, forming the roof of the subacromial space.
- Bursa:
- The subacromial bursa is a fluid-filled sac that reduces friction between the acromion and the rotator cuff tendons.
Role of the Acromion and Rotator Cuff
The acromion and the rotator cuff play critical roles in shoulder mechanics and are directly involved in the development of shoulder impingement syndrome.
- The Acromion:
- This bony projection of the scapula forms the roof of the shoulder, creating the subacromial space where tendons and the bursa reside.
- Its shape—flat, curved, or hooked—can influence the likelihood of impingement. A hooked acromion, for example, narrows the subacromial space, increasing the risk of compression and irritation of the rotator cuff tendons.
- During shoulder movements, the acromion must glide smoothly over the tendons and bursa to prevent friction. Any disruption, such as bone spurs or inflammation, can exacerbate impingement.
- The Rotator Cuff:
- This group of four muscles stabilizes the shoulder joint by keeping the humeral head centered in the glenoid socket during motion.
- It enables precise movements like lifting the arm and rotating it in multiple directions.
- Overuse, poor posture, or aging can lead to wear and tear on the rotator cuff tendons, causing inflammation or partial tears. This not only reduces shoulder mobility but also increases the likelihood of impingement as the tendons are compressed within the subacromial space.
What is Shoulder Impingement Syndrome?
Shoulder impingement syndrome is a common condition that occurs when the soft tissues in the shoulder, such as tendons or the bursa, become compressed or irritated. This compression usually happens in the subacromial space—the narrow area between the acromion (a bony projection of the shoulder blade) and the rotator cuff tendons. Over time, this mechanical impingement can lead to pain, inflammation, and reduced mobility, particularly during overhead activities.
Definition and Mechanism
At its core, shoulder impingement syndrome is a repetitive strain injury caused by prolonged or repeated compression of soft tissues in the shoulder. The primary structures involved are:
- Rotator Cuff Tendons: These are responsible for stabilizing the shoulder joint and facilitating movement. Impingement can cause irritation, inflammation, or even tears in these tendons.
- Subacromial Bursa: This fluid-filled sac cushions the tendons as they move. Inflammation of the bursa, known as bursitis, often accompanies impingement and exacerbates the condition.
During arm elevation, such as lifting, reaching, or throwing, the humeral head (upper arm bone) naturally moves closer to the acromion. Normally, this motion occurs without friction due to adequate space and smooth interaction between the tissues. However, in shoulder impingement syndrome, this space becomes narrowed, causing the soft tissues to become compressed. This narrowing can occur due to several factors:
- Structural Factors:
- Acromion Shape: A hooked or curved acromion reduces the subacromial space and increases the risk of impingement.
- Bone Spurs: Bony growths on the acromion can further decrease space and irritate the tendons.
- Functional Factors:
- Muscle Imbalance: Weakness or poor coordination in the rotator cuff muscles may lead to improper positioning of the humeral head, causing impingement.
- Overuse: Repetitive overhead motions can strain the rotator cuff tendons, leading to swelling and narrowing of the subacromial space.
Risk Factors
Certain individuals are more likely to develop shoulder impingement syndrome due to specific lifestyle or physical factors. These risk factors include:
- Athletic Activities:
- Athletes participating in sports requiring repetitive overhead motions, such as volleyball, basketball, or gymnastics, are at high risk.
- Swimmers, often referred to as having “swimmer’s shoulder,” frequently experience impingement due to the repetitive arm movements involved in strokes.
- Occupational Hazards:
- Jobs involving heavy lifting, prolonged overhead work, or repetitive shoulder use can lead to chronic strain and eventual impingement.
- Poor Shoulder Mechanics:
- Weakness in the rotator cuff muscles or poor scapular control can lead to instability, improper joint alignment, and greater susceptibility to impingement.
- Previous Injuries:
- Individuals who have experienced shoulder injuries, such as rotator cuff tears or dislocations, are more prone to developing impingement syndrome.
- Age:
- The condition is most common in individuals over 40, as age-related changes in tendon strength, elasticity, and joint space naturally occur.
- Postural Problems:
- Sedentary lifestyles and excessive time spent sitting (e.g., at a desk) can lead to postural imbalances that predispose individuals to impingement.
Structures that are part of the creation of the coracoacromial arch
The shoulder comprises several key structures, including the coracoacromial arch, rotator cuff tendons, and subacromial bursa. The coracoacromial arch, formed by the coracoid process, the acromion, and the coracoacromial ligament, plays a pivotal role in shoulder movement and stability. Compression of these structures leads to inflammation and pain, characteristic of SAIS.
- Coracoid process: This is a bony protrusion located at the front of the scapula (shoulder blade). The coracoid process plays a key role in the formation of the coracoacromial arch.
- Acromion: The acromial process is an extension of the scapula that articulates with the clavicle to form the acromioclavicular joint. The acromion is another important component of the coracoacromial arch.
- Coracoacromial ligament: This ligament strengthens the subacromial space and forms, with the acromion and the coracoid process, a protective arch above the head of the humerus.
- Subacromial bursa: Although not a bony structure, the subacromial bursa, a fluid-filled sac, is also part of the whole. It lies between the acromion and the supraspinatus muscle tendon, helping to reduce friction during shoulder movement.
These components collectively form the coracoacromial arch, which, along with other shoulder structures, helps create a stable and functional environment for arm movement. Abnormalities or changes in these structures can contribute to problems such as subacromial impingement, a condition where the subacromial space is reduced, potentially leading to pain and impairments in shoulder movement.
Structures that can be compressed
Below the coracoacromial arch, which is formed by the acromion, coracoid process, and coracoacromial ligament, several anatomical structures may be subject to compression. This compression can lead to problems such as subacromial impingement. Structures that may be compressed under the arch (acromion) include:
- Rotator Cuff Muscle Tendons: The tendons of the supraspinatus, subscapularis, infraspinatus, and teres minor muscles are particularly vulnerable to compression below the coracoacromial arch. Subacromial impingement can lead to irritation, inflammation, and even tears of these tendons.
- Subacromial bursa: The subacromial bursa, located between the acromion and the tendon of the supraspinatus muscle, can also be compressed. Inflammation of this bursa (bursitis) is common in subacromial impingement.
- Coracoacromial ligament: Although this ligament is an integral part of the coracoacromial arch, excessive ossification or hypertrophy of this ligament can contribute to compression of underlying structures.
- Suprascapular nerve: This nerve passes close to the coracoacromial arch. Excessive compression can lead to symptoms such as pain and weakness in the shoulder area.
- Acromial artery: Although less common, the acromial artery, which supplies blood to the acromion, can become compressed, leading to circulatory problems in the area.
A little history
Shoulder impingement, a concept developed by Neer in 1972, provides a crucial explanation for understanding pathology involving the shoulder region. According to this theory, it is characterized by compression of the soft tissues, in particular the supraspinatus tendon and the subacromial bursa, between the underside of the acromion (linked to the acromioclavicular joint or the coracoacromial ligament ) and the humeral head, especially during arm elevation movements.
Shoulder impingement arises from a complex anatomical interaction between the different structures of the shoulder. The acromion, a bony protrusion of the shoulder blade, and the humeral head, the arm bone, play a central role in this mechanism. When the arm is elevated, these two structures come into contact, creating a restricted space where the soft tissues can be compressed. This occurs particularly during arm elevation movements, thus involving the supraspinatus tendon and the subacromial bursa.
According to Neer, shoulder impingement is attributed to excessive compression during these movements, which can have serious consequences. Notably, Neer puts forward the idea that this conflict is responsible for 93% of rotator cuff tears. The rotator cuff is a collection of muscles and tendons crucial for stability and movement of the shoulder. Thus, repeated and excessive compression of these structures during shoulder impingement can lead to damage, inflammation and eventually tears in the rotator cuff.
Understanding shoulder impingement is of major importance in the field of orthopedics and sports medicine. Practitioners use this conceptualization to diagnose and treat shoulder disorders, with a focus on managing factors contributing to soft tissue compression. Treatment approaches may include conservative methods such as physical therapy, as well as surgical interventions in more severe cases.
Causes
- Tendon inflammation: Inflammation of the rotator cuff tendons, which are responsible for shoulder stability, can contribute to subacromial syndrome.
- Repetitive movements: Activities that involve repetitive arm movements, especially arm elevation movements, can cause excessive wear and tear on the tendons and contribute to the syndrome.
- Anatomical abnormalities: Anatomical abnormalities, such as particular shapes of the acromial bone, can reduce the space available for the tendons, increasing the risk of subacromial impingement.
- Previous injuries: Previous injuries to the shoulder, such as sprains or fractures, can alter the normal structure of the shoulder, allowing the syndrome to develop.
- Poor posture: Improper posture, especially during repetitive activities, can contribute to compression of the tendons beneath the acromial bone.
- Muscle weakness: Weakness in the muscles surrounding the shoulder can lead to instability, increasing the risk of tendon friction and irritation.
- Age: Aging can lead to tendon degeneration, increasing susceptibility to subacromial syndrome.
- Joint disorders: Certain joint disorders, such as shoulder arthritis, may contribute to the development of the syndrome.
The structures most vulnerable to impingement between the lower surface of the acromion and the head of the humerus are the greater tuberosity, the overlying supraspinatus tendon, and the long head of the biceps. The main site of compression is anterior to the acromion angle. This is why the correct term is anterior impingement syndrome.
Symptoms
Gradual onset of anterior and lateral shoulder pain exacerbated by overhead activity is characteristic. Nighttime pain and difficulty sleeping on the affected side are also common. Atrophy of the muscles at the top and back of the shoulder may be apparent if the patient has had symptoms for several months.
- Shoulder pain: Pain is the main symptom. It is usually felt in the upper and front part of the shoulder. The pain may radiate down the arm, especially during specific movements, such as raising the arm to the side.
- Pain during arm elevation: A sharp pain or “painful arc” may be felt when raising the arm to the side, especially between 40 and 120 degrees of elevation. Pain associated with subacromial impingement typically manifests during shoulder abduction, occurring most commonly in the range of motion between 40 and 120 degrees. This conflict, often linked to anatomical anomalies or a reduction in the subacromial space, leads to compression of the tendons of the supraspinatus muscle and the bursa, thus generating specific painful discomfort.
- Nighttime pain: Some individuals may experience increased pain at night, particularly when trying to sleep on the affected side.
- Muscle weakness: Due to pain and irritation of the tendons, there may be perceived weakness in the affected arm.
- Difficulty lifting heavy objects: Activities that require arm elevation, especially with heavy objects, can be difficult and painful.
- Crepitus or clicks: Some patients may experience a crepitus or click sensation during shoulder movement.
- Stiffness: Shoulder stiffness may be felt, limiting range of motion.

Mechanism of subacromial impingement syndrome
Subacromial impingement syndrome (SAIS) involves a complex mechanism of compression and irritation of structures beneath the acromial bone, primarily the rotator cuff tendons. H
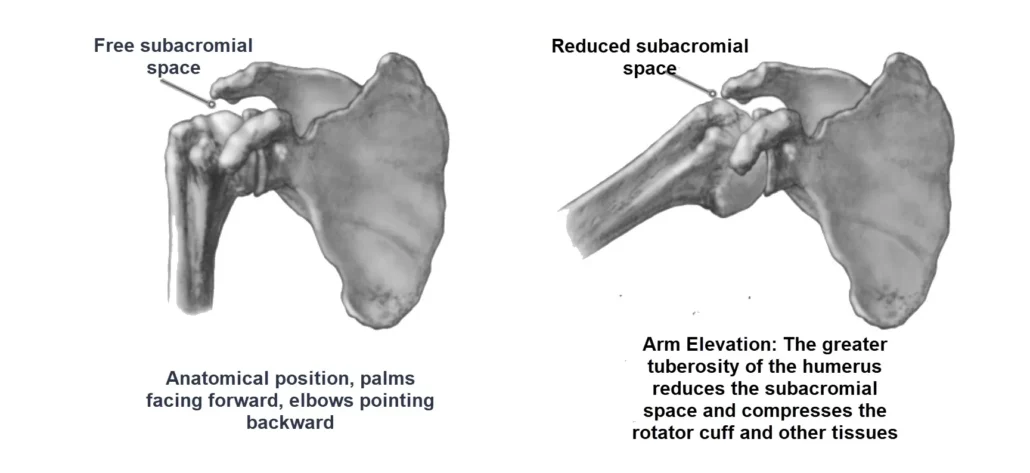
Left Arm (Anatomical Position): The subacromial space is open, indicating no compression of the rotator cuff tendons.
Right Arm (Elevation): The elevation of the arm causes the greater tuberosity of the humerus to encroach upon the subacromial space, leading to compression of the rotator cuff tendons. This illustrates a key aspect of shoulder impingement syndrome, where the reduced space can cause pain and restricted movement.
The anatomical nuances of the acromion (anatomical anomaly)
Variations in acromion types play a crucial role in shoulder physiology and may influence the development of certain pathological conditions. In general, there are three main types of acromion.
The first type (type 1) is characterized by a flat underside. This means that the lower portion of the acromion is relatively straight, providing adequate space for the tendons and subacromial bursa. In the majority of individuals, this anatomical configuration prevails.
However, some have a second type of acromion (type 2) with a curved underside. This curvature can reduce the space available under the acromion, which can potentially lead to compression of the supraspinatus and bursa tendons. People with type 2 acromion may therefore be more predisposed to problems such as subacromial impingement and associated pain.
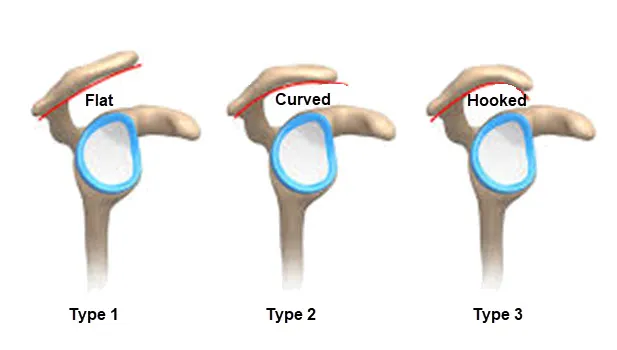
Type 1 (Flat Acromion): Characterized by a flat undersurface, providing adequate space beneath the acromion, thus reducing the likelihood of subacromial impingement.
Type 2 (Curved Acromion): Features a curved underside, which reduces the subacromial space. This anatomical variation increases the risk of subacromial impingement and can lead to discomfort and pain.
Type 3 (Hooked Acromion): Exhibits a hooked underside, creating a significantly restricted subacromial space. This type is associated with greater compression of the rotator cuff tendons, often leading to increased pain and discomfort
The third type of acromion (type 3) is characterized by a hooked underside. In this case, the curvature is more pronounced, creating an even more restricted space for the tendons and bursa. Individuals with a type 3 acromion are likely to experience greater compression, increasing the risk of pain and discomfort in the shoulder area.
It is important to note that variability in acromion types may have clinical implications, particularly in the context of subacromial impingement. When the subacromial space is reduced due to the morphology of the acromion, this can contribute to the development of conditions such as supraspinatus tendinopathy and bursitis.
In summary, the diversity of acromion types plays a vital role in understanding potential problems in the shoulder, providing important insights for healthcare professionals working in the field of orthopedics and osteopathy. .
Clinical Presentations
Stages of Neer impaction syndrome
The stages of Neer impaction syndrome describe the progression of the condition based on damage to the rotator cuff tendons. Here is a brief description of the three stages of Neer impaction syndrome:
- Stage I:
- Description: This stage is characterized by edema (swelling) and hemorrhage in the rotator cuff tendons.
- Manifestations: The patient may feel pain when raising the arm, but there may not be an obvious tendon tear at this stage.
- Stage II:
- Description: The lesions progress with the appearance of partial tears of the rotator cuff tendons.
- Manifestations: The pain becomes more persistent and may be felt during the night. Shoulder movements may be limited.
- Stade III :
- Description: This stage is characterized by complete tears of the rotator cuff tendons.
- Manifestations: The pain is more intense and may be present even at rest. Loss of shoulder strength and mobility is more evident.
Clinical Tests Used to Evaluate Shoulder Impingement Syndrome
These tests involve evaluating specific movements and replicating conditions that may cause symptoms associated with impingement.
- Test the Down:
- Description: The examiner passively raises the patient’s arm into forward flexion.
- Positive Outcome: Pain or discomfort during movement may indicate impingement.
- Test the Hawkins-Kennedy:
- Description: The examiner actively internally rotates the patient’s arm while raising it forward.
- Positive Outcome: Pain or discomfort during internal rotation may suggest impingement.
- Empty Can Test (Jobe Test):
- Description: The patient raises the arms 90 degrees in the scapular plane with the thumbs pointing down, and resistance is applied.
- Positive result: Pain or weakness during resisted abduction may indicate impingement of the supraspinatus muscle.
- Drop Arm Test:
- Description: The patient is asked to actively lower the arm from an abducted position.
- Positive Outcome: Inability to lower the arm smoothly and actively may indicate a tear or weakness of the supraspinatus muscle.
- Yocum test:
- Description: The patient’s arm is placed in maximum forward flexion with an axial load applied by the longitudinal axis of the humerus.
- Positive Outcome: Pain or discomfort during this maneuver may suggest acromioclavicular joint pathology or impingement.
- External Rotation Resistance Test (ERST):
- Description: The patient’s arm is externally rotated against resistance.
- Positive result: Pain or weakness during resisted external rotation may indicate impingement of the infraspinatus or teres minor muscles.
- Cross Adduction Test (Crossed Arms Test):
- Description: The patient brings the arm to the chest.
- Positive result: Pain during this movement may indicate pathology of the acromioclavicular joint or impingement.
- Painful Arc Test:
- Description: The patient actively raises the arm, and the examiner observes if there is a painful arc during the range of motion.
- Positive result: Pain during a specific range of abduction may suggest impingement.
Neer Test:
The Neer Test is a clinical test used to assess the presence of pain or discomfort associated with possible shoulder impingement syndrome. Here is how it is generally done:
- The patient is generally in a standing or seated position, with the arm on the side to be tested completely relaxed alongside the body.
- The examiner stands behind the patient and firmly grasps the patient’s arm at the wrist.
- The examiner slowly raises the patient’s arm into anterior flexion, so that the arm gradually approaches the patient’s head.
- The movement continues until the arm is completely elevated.
Test Result: A positive result is indicated if the patient experiences pain or discomfort during movement, usually in the anterior or upper shoulder region.
Interpretation: Pain during the Neer Test may indicate possible irritation or impingement of the supraspinatus muscle tendons below the acromion, which is characteristic of shoulder impingement syndrome.
It is important to note that the results of clinical tests, including the Neer Test, must be interpreted in the context of the patient’s history, other clinical examinations and possibly medical imaging to make an accurate diagnosis and determine the appropriate treatment plan. This test is generally carried out by health professionals such as doctors or orthopedists.
Test the Hawkins-Kennedy
The Hawkins sign is a clinical test used to evaluate the presence of subacromial impingement in the shoulder. It is often performed as part of the physical exam to identify possible problems such as subacromial impingement syndrome. Here is how the test is generally performed:
- Patient position: The patient is usually in a sitting or standing position.
- Practitioner Position: The practitioner elevates the patient’s arm to approximately a 90 degree angle in the frontal plane (forward elevation) and flexes the elbow to 90 degrees.
- Manipulation: The practitioner then performs a forced internal rotation of the patient’s arm by rotating the forearm inwards.
- Interpretation: If the movement causes pain in the subacromial region, it is considered a positive Hawkins sign, suggesting possible subacromial impingement.
The Hawkins sign is often used in conjunction with other clinical tests and evaluations to obtain a more complete diagnosis of shoulder problems. A positive result may indicate irritation or compression of subacromial structures, such as the rotator cuff tendons or subacromial bursa.
It is important to note that the Hawkins sign, although useful in the initial evaluation, is not a definitive diagnosis, and other medical tests, such as medical imaging (MRI, x-rays), may be necessary to confirm and further characterize the underlying issues.

- Pain at 90° of forward flexion with forced internal rotation (results in greater tuberosity under the coracoacromial ligament). It is important to document rotator cuff strength.
Types
- Primary (more common): the impingement here occurs under the arch of the acromio-coracoid arch and is due to subacromial overload.
- Secondary : It is due to a relative decrease in the subacromial arch and is due to microinstability of the glenohumeral joint or scapulothoracic instability.
- Posterior (internal): Appears in athletes who work overhead such as throwers, swimmers and tennis players. The supraspinatus and infraspinatus tendons are trapped between the posterior and superior aspects of the glenoid when the arm is in an elevated position and externally rotated.
Understanding the role of osteopathy in the treatment of subacromial impingement
- Overall Patient Assessment: Osteopaths perform a comprehensive assessment of the patient, taking into account not only shoulder-specific symptoms, but also the entire body. They seek to understand postural imbalances, movement restrictions and possible contributing factors.
- Correction of postural imbalances: Osteopaths can work on improving the patient’s posture, as postural imbalances can contribute to the development of subacromial impingement. Manual adjustments and specific exercises may be prescribed to restore alignment and reduce pressure on the shoulder.
- Release of muscle tension: Osteopaths use muscle release techniques to reduce tension in the muscles surrounding the shoulder. This can help improve blood circulation, reduce inflammation and promote healing.
- Patient Education: Osteopaths often play an educational role by advising patients on specific exercises, lifestyle modifications, and self-care techniques that can contribute to the long-term management of subacromial impingement.
Stretches and Exercises for Patients With Subacromial Impingement
Sleeper Stretch
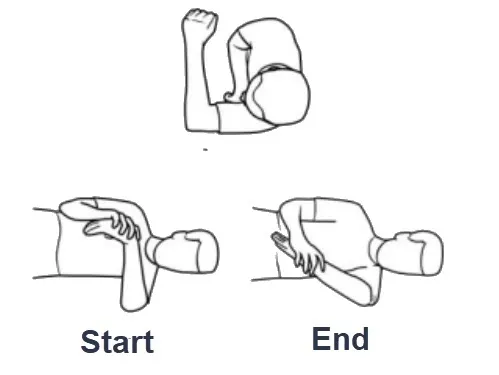
- Lie on your side on a firm, flat surface with the affected shoulder beneath you and the arm positioned as shown, keeping your back perpendicular to the surface.
- With the unaffected arm, push the other wrist down toward the surface. wrist downwards, toward the surface. Stop when you feel a stretching sensation at the back of the affected shoulder.
- Hold this position for 30 seconds, then relax the arm for 30 seconds.
- Perform 3 or 4 sets of 4 repetitions per day, continuing for 3 to 4 weeks.
Rotation externe

- Lie on your side on a firm, flat surface with the unaffected arm underneath you, cradle your head.
- Hold the affected arm against your side as shown, with the elbow bent at a 90° angle.
- Slowly rotate the arm at shoulder level, keeping the elbow bent and against your
- side, to raise the weight to an upright position, then slowly lower the weight to the starting position for a count of 5.
- Start with weights of around 1 to 2 pounds. weights that allow 2 sets of 8 repetitions, progressing up to 3 sets of 15 repetitions.
- Add weight in 1-pound increments, starting again at each new weight level with 2 sets of 8 repetitions, up to a maximum of 3 to 6 pounds, depending on your size and needs. 6 pounds, depending on your height and fitness level.
- Perform the exercise 3 or 4 days a week, continuing for 6 to 8 weeks.
Internal rotation

- Lie on your side on a firm, flat surface with the affected arm underneath you and with a pillow or folded cloth under your head to keep your spine straight.
- Hold the affected arm against your side as shown, with the elbow bent at a 90° angle.
- Slowly rotate the arm at shoulder level, keeping the elbow bent and against your torso, to raise the weight to a vertical position, then slowly lower the weight to the starting position.
- Start with weights that allow 2 sets of 8 repetitions. 8 repetitions, progressing to 3 sets of 15 repetitions.
- Add weight in 1-pound increments, starting again at each new weight level with 2 sets of 15 repetitions. Start again at each new weight level with 2 sets of 8 repetitions, up to a maximum of 3 to 6 pounds, depending on your size and needs. 6 pounds, depending on your height and fitness level.
- Perform the exercise 3 or 4 days
Conclusion
Subacromial impingement syndrome (SAIS) represents a common challenge for many individuals, leading to significant pain and functional limitations in the shoulder. Osteopathy positions itself as an essential holistic and complementary approach in the management of this disorder. With a focus on thorough assessment, correction of muscular imbalances, and the use of specific manual therapy techniques, osteopaths aim to relieve compression, restore mobility, and promote healing.
It is crucial to emphasize that osteopathic treatment must be personalized according to the individual needs of each patient. Preventive approaches and advice on stretching and exercises also contribute significantly to improving the condition and preventing relapses.
By exploring these aspects, individuals can find osteopathy a comprehensive solution to alleviate pain, restore function and promote long-term health of the shoulder. Osteopaths, with their in-depth expertise of the human body, play a key role in the care team for people suffering from subacromial impingement syndrome, providing a patient-centered approach to promoting well-being and quality of life. life.
References
- Nazari G, MacDermid JC, Bryant D, Athwal GS. The effectiveness of surgical vs conservative interventions on pain and function in patients with shoulder impingement syndrome. A systematic review and meta-analysis. PLoS One. 2019;14(5):e0216961. [PMC free article] [PubMed]
- Consigliere P, Haddo O, Levy O, Sforza G. Subacromial impingement syndrome: management challenges. Orthop Res Rev. 2018;10:83-91. [PMC free article] [PubMed]
- Lewis JS. Rotator cuff tendinopathy/subacromial impingement syndrome: is it time for a new method of assessment? Br J Sports Med. 2009 Apr;43(4):259-64. [PubMed]
- Davis DD, Nickerson M, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Feb 12, 2022. Swimmer’s Shoulder. [PubMed
- Varacallo M, Tapscott DC, Mair SD. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Feb 12, 2022. Superior Labrum Anterior Posterior Lesions. [PubMed]
- Varacallo M, El Bitar Y, Mair SD. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Feb 12, 2022. Rotator Cuff Syndrome. [PubMed]
- Credit in part: Julie A. Creech; Sabrina Silver


















{kind=link}