
")
Introduction
Anterior shoulder instability, also known as anterior shoulder instability, is an orthopedic condition that is characterized by excessive looseness of the shoulder joint on the frontal side. This condition can occur from a variety of causes, including trauma, sports injuries, or overuse of the shoulder in repetitive activities.
The dynamics of the shoulder joint are complex, involving an interaction between muscles, ligaments and bony structures. When this harmony is disrupted, anterior instability of the shoulder can develop, exposing the patient to the risk of dislocation of the joint.
The prevalence of anterior shoulder instability varies, but it is often seen in individuals participating in athletic activities, including contact sports or sports requiring intense shoulder movement, such as tennis or baseball. . People who are genetically predisposed to having looser ligaments may also be more prone to this condition.
Symptoms of anterior shoulder instability may include a feeling of dislocation or sliding of the shoulder, persistent pain, muscle weakness, and decreased stability of the joint. These symptoms can significantly affect the patient’s quality of life, leading to limitation of daily activities and sports.
Diagnosis of this condition is based on a thorough clinical evaluation, a patient’s medical history, and imaging studies such as x-rays or magnetic resonance imaging (MRI). Once diagnosed, treatment may vary depending on the severity of the instability.
Treatment approaches may include physical therapy to strengthen the muscles surrounding the shoulder, joint stabilization exercises, and behavioral modifications to minimize the risk of dislocation. In more severe or recurring cases, surgery may be considered to repair loose or damaged structures in the shoulder.
In addition to the medical aspects, anterior shoulder instability can have psychological repercussions, affecting the patient’s confidence in their physical abilities. Sufferers may feel apprehensive about performing certain movements for fear of causing a dislocation.
To overcome these challenges, psychological and emotional support can be essential in the rehabilitation process. Patients can benefit from a holistic approach that integrates physical rehabilitation and psychological care to promote full recovery.
Important Warning:The information on this blog is for educational purposes only and not a substitute for professional medical advice. Do not attempt any maneuvers, exercises, or treatments described here without consulting a qualified healthcare professional. Improper application may lead to injury or complications. Always seek professional guidance for your specific health needs.
Causes
- Labral Injuries: Injuries to the glenoid labrum, a cartilaginous structure that surrounds the shoulder joint, are a common cause of anterior instability. A tear or damage to the labrum can compromise the stability of the joint.
- Strained or Ruptured Ligaments: The shoulder ligaments play a crucial role in joint stability. Excessive elongation or rupture of ligaments, particularly the inferior glenohumeral ligament, can lead to anterior instability.
- Loose Joint Capsule: A joint capsule that is too loose can result from genetic factors or acquired laxity over time. A loose capsule does not provide the necessary support to the joint, thus promoting instability.
- Glenoid Dysplasia: Congenital glenoid dysplasia, where the glenoid socket is abnormally shallow, can create an environment conducive to shoulder instability.
- Trauma: Trauma such as anterior shoulder dislocations, falls or accidents can damage anatomical structures, contributing to instability.
- Repetitive Activities: Sports or work activities that involve repetitive overhead arm movements, such as throwing, may contribute to anterior shoulder instability.
- Muscle Weakness: Weakness of the stabilizing muscles of the shoulder, particularly the rotator cuff muscles, can compromise the stability of the joint.
- Multidirectional Instability: Some people may experience multidirectional instability, where the joint is vulnerable to movement in multiple directions, including forward.
- Medical Conditions: Medical conditions such as joint hyperlaxity, accessory nerve palsy, or hyperlaxity syndrome may increase the risk of anterior shoulder instability.
- Genetic Factors: Some individuals may have a genetic predisposition to develop shoulder instability due to anatomical variations or tissue laxity.
- Poor Posture: Poor posture, particularly a forward shoulder position, can contribute to overuse of some muscles and weakness in others, thereby promoting instability.
Symptoms
- Pain: Pain is one of the most common symptoms of anterior shoulder instability. This pain can be felt in the front of the shoulder and can be triggered by specific movements or physical activities.
- Sensation of Dislocation or Subluxation: People with anterior shoulder instability may experience a sensation of dislocation or subluxation, where the joint seems to slide partially out of its normal position. This sensation can occur during specific movements or even at rest.
- Crepitation or Rattling: Some individuals may hear or feel noises such as crackling or clicking when they move their shoulder. These sounds may be associated with abnormal friction of the joint surfaces.
- Muscle Weakness: Muscle weakness, particularly in the rotator cuff muscles, may accompany anterior shoulder instability. This may affect the ability to perform specific movements or lift objects.
- Inability to Raise Arm Safely: Some individuals may experience an inability to safely raise their arm overhead without fear of instability or increased pain.
- Numbness or Tingling: Sensations of numbness or tingling may occur in the shoulder or arm area. This may be the result of nerve irritation due to instability.
- Limitation of Mobility: Anterior instability of the shoulder can lead to limited mobility, particularly during arm elevation, abduction or rotation movements.
- Frequent Dislocation or Dislocation Episodes: Some individuals may experience frequent episodes of complete shoulder dislocation, often requiring manual reduction to reposition the joint.
- Pressure Sensitivity: The anterior shoulder region may be sensitive to pressure, and palpation of this area may trigger pain or discomfort.
- Muscle Fatigue: Increased muscle fatigue may be experienced, particularly when performing tasks requiring constant stabilization of the shoulder.
Pathophysiology
The pathophysiology of anterior shoulder instability is an essential component to understanding how this condition develops and progresses. This in-depth description of the underlying mechanisms may help guide treatment approaches and better understand the potential complications associated with this orthopedic condition.
Anterior shoulder instability usually results from a disruption of the delicate balance between the anatomical structures that stabilize the shoulder joint. This joint, also called the glenohumeral joint, is formed by the head of the humerus and the glenoid cavity of the scapula. The main factors involved in the pathophysiology of anterior shoulder instability include the ligaments, muscles, and joint capsule.
- Ligaments: Ligaments play a crucial role in maintaining the stability of the shoulder joint. When there is excessive stretching or tearing of these ligaments, particularly the inferior glenohumeral ligament, it can lead to instability. Acute trauma, such as recurrent dislocations or sprains, can contribute to these ligament injuries.
- Muscles: The muscles surrounding the shoulder, particularly the rotator cuff muscles, help stabilize the joint. A muscular imbalance, often characterized by muscle weakness or dominance, can compromise this stability. For example, weakness in the rotator cuff muscles can increase the risk of anterior instability.
- Joint Capsule: The joint capsule is a connective tissue that surrounds the shoulder joint. Changes in the structure or elasticity of the capsule can influence the stability of the joint. Traumatic events or repetitive movements can cause capsule laxity, contributing to instability.
- Traumatic Mechanisms: Trauma, such as recurrent shoulder dislocations, can create damage to ligaments, muscles and other structures. These repeated injuries can initiate a vicious cycle of instability, with each episode of dislocation further damaging the stabilizing structures.
- Variant Anatomy: Some individuals may have varying shoulder anatomy, such as a more shallow glenoid fossa, which may predispose to instability.
- Triggering Events: Certain triggering events, such as sudden movements, accidents or heavy loads, can contribute to the appearance of instability. These events can create excessive force on the shoulder joint, exceeding its normal stabilizing capacity.
Shoulder Laxity Category
- Traumatic Laxity: This category concerns laxity that results from injury or direct trauma to the shoulder. Ligament sprains, shoulder dislocations, and other injuries related to accidents or falls can lead to traumatic laxity.
- Atraumatic Laxity: Atraumatic laxity occurs without any apparent injury or trauma. It can be caused by factors such as anatomical abnormalities, genetic disorders, connective tissue disorders, or muscle imbalances.
- Anterior Laxity vs. Posterior Laxity: Depending on the direction in which the laxity is more pronounced, we can distinguish anterior shoulder laxity (more common) from posterior laxity. Anterior laxity can often result from traumatic injuries, while posterior laxity may be associated with specific shoulder mechanisms.
- Overall Laxity vs. Partial Laxity: Overall shoulder laxity indicates extensive laxity involving multiple structures, while partial laxity may be more localized, affecting a specific part of the shoulder.
- Congenital Laxity: Some people may have shoulder laxity from birth due to genetic factors or congenital conditions. In such cases, laxity may be present from early in life and may require special management.
- Symptomatic vs. Asymptomatic Laxity: Shoulder laxity may be symptomatic, causing pain, instability, or other symptoms, or it may be asymptomatic, causing no noticeable discomfort to the patient.
Anterior shoulder dislocation
An anterior shoulder dislocation is usually caused by a blow to the arm that is abducted, externally rotated, and extended (for example, blocking a basketball shot). More rarely, a blow to the posterior humerus or a fall on an outstretched arm can cause an anterior dislocation.
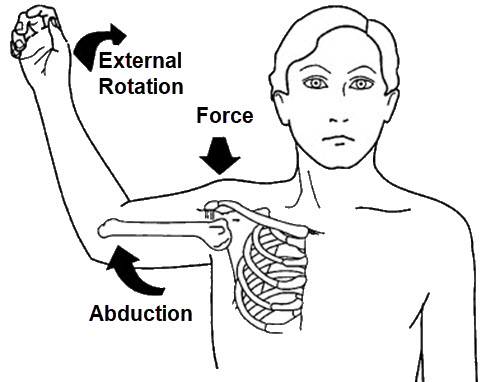
The illustration demonstrates three key elements leading to dislocation:
Abduction: The arm is positioned away from the body, opening the shoulder joint and placing it in a vulnerable position.
External Rotation: The arm is rotated outward, which further destabilizes the humeral head and shifts it toward the anterior edge of the joint.
Force: A downward or forward force applied to the shoulder can push the humeral head out of the glenoid cavity, leading to the dislocation.
The arm is generally held in a position of abduction and external rotation. There is loss of the normal contour of the deltoid and the acromion is prominent posteriorly and laterally. The humeral head itself may well be palpable anteriorly.
Upon closer examination, there may be specific damage to the bone, vascular and nerve structures in the area. It is important to record neurovascular status before attempting reduction. In the longer term, a rotator cuff injury may also occur.
Reduction of anterior shoulder dislocations using the Spaso technique
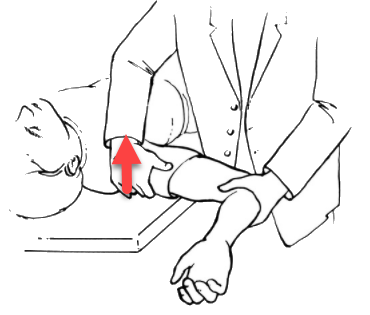
The Spaso technique is a commonly used technique for the reduction of anterior shoulder dislocation in the injured without anesthesia. It consists of forward flexion, external rotation and gentle traction for the reduction of anterior shoulder dislocations with the patient in supine position (lying on the back).
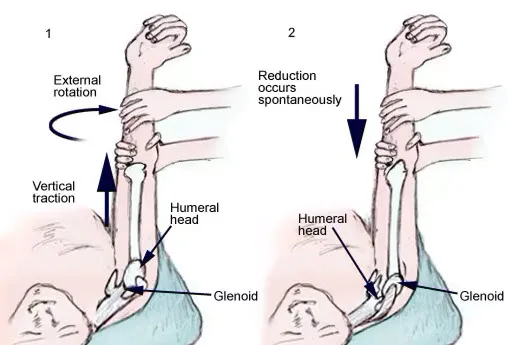
In the first step, the arm is gently pulled to apply vertical traction, aligning the humerus with the glenoid cavity. Simultaneously, external rotation is applied to the arm, which helps to disengage the humeral head from any obstructive positioning in the joint. This maneuver reduces muscle tension around the shoulder, easing the reduction process.
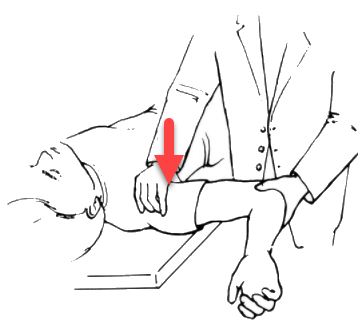
The second step demonstrates the spontaneous reduction of the humeral head back into the glenoid cavity. As the arm is carefully rotated outward and traction is maintained, the humeral head naturally repositions itself into its anatomical alignment within the joint. This step is often accompanied by a noticeable “clunk” or release as the shoulder relocates.
This technique minimizes the risk of additional damage to surrounding tissues, ligaments, or nerves. It is a commonly used method in emergency and orthopedic settings due to its simplicity and effectiveness. Proper technique and patient relaxation are crucial to ensure a successful and pain-minimized reduction.
Laxity Test – Hawkins Classification
The Hawkins Laxity Test is a specific assessment aimed at measuring shoulder stability by categorizing the different degrees of displacement of the humeral head relative to the glenoid. Here is a clearer description of each grade:
Grade 1: No Movement
The humeral head shows no significant signs of displacement relative to the glenoid, indicating normal shoulder stability.
Grade 2: Light Upward Movement
The humeral head shows a slight upward displacement of the glenoid. Although noticeable, this displacement remains moderate, indicating slight laxity of the shoulder joint.
Grade 3: Subluxation (Displacement towards the Edge of the Glenoid)
The humeral head rises towards the edge of the glenoid without, however, completely exceeding it. This grade is characterized by subluxation, where the humeral head exhibits notable displacement without completely dislocating from the glenoid.
Grade 4: Dislocation (Complete Displacement)
The humeral head rises and completely covers the edge of the glenoid. This grade indicates a complete dislocation, associated with severe shoulder instability.
This classification allows healthcare professionals to objectively assess the degree of shoulder laxity, making it easier to adapt the treatment plan based on the severity of the condition. Importantly, this assessment, combined with other tests and the patient’s medical history, contributes to a holistic understanding of the shoulder condition, thereby guiding treatment decisions.
Anterior Glenohumeral Instability Tests The anterior drawer test is a clinical test used to evaluate anterior glenohumeral instability of the shoulder. This test is commonly used in the medical field to evaluate the laxity of the ligamentous structures of the shoulder. Here is how the anterior drawer test is typically performed:
Anterior Drawer Test Procedure:
- Patient Position: The patient is usually seated or standing, with the arm in question placed in a specific position.
- Tester Position: The healthcare professional performing the test stands behind the patient.
- Stabilization: The tester stabilizes the patient’s scapula by placing one hand on the shoulder blade, while holding the shoulder in a specific position.
- Movement: With the other hand, the tester grasps the patient’s arm at the forearm and applies forward force, simulating the movement of an “anterior drawer.” This aims to move the humeral head anteriorly relative to the glenoid fossa.
- Assessment: During the movement, the tester observes the patient’s reactions, including any apprehension, pain, or sensation of dislocation. The test can also be performed at different ranges of motion to assess laxity.
Interpretation:
- Positive: A positive test may indicate excessive laxity of the anterior ligamentous structures of the shoulder, suggesting possible anterior glenohumeral instability.
- Negative: A negative test suggests normal shoulder stability during anterior drawer movement.
Posterior glenohumeral instability testing
The posterior drawer test is a clinical examination used to evaluate posterior glenohumeral instability of the shoulder. It is one of the tests that can be performed during a complete assessment of shoulder stability. Here is how the posterior drawer test is typically performed:
Posterior Drawer Test Procedure:
- Patient Position: The patient is usually seated or standing.
- Tester Position: The healthcare professional performing the test positions himself behind the patient.
- Stabilization: The tester stabilizes the patient’s scapula (shoulder blade) by placing one hand on the shoulder blade, while holding the shoulder in a specific position.
- Movement: With the other hand, the tester grasps the patient’s arm at the forearm and applies force backwards, simulating the movement of a “posterior drawer.” This aims to move the humeral head posteriorly relative to the glenoid fossa.
- Assessment: During the movement, the tester observes the patient’s reactions, including any apprehension, pain or sensation of dislocation. The test can also be performed at different ranges of motion to assess laxity.
Interpretation:
- Positive: A positive test may indicate excessive laxity of the posterior ligamentous structures of the shoulder, suggesting possible posterior glenohumeral instability.
- Negative: A negative test suggests normal shoulder stability during posterior drawer movement.
Posterior Drawer Test
References
- Gottschalk LJ, Walia P, Patel RM, Kuklis M, Jones MH, Fening SD, Miniaci A. Stability of the Glenohumeral Joint With Combined Humeral Head and Glenoid Defects: A Cadaveric Study. Am J Sports Med. 2016 Apr;44(4):933-40. [ PubMed ]2.
- Cofield RH, Kavanagh BF, Frassica FJ. Anterior shoulder instability. Instr Course Reading 1985;34:210-27. [ PubMed ]3.
- Walton J, Paxinos A, Tzannes A, Callanan M, Hayes K, Murrell GA. The unstable shoulder in the adolescent athlete. Am J Sports Med. 2002 Sep-Oct;30(5):758-67. [ PubMed ]4.
- Joseph TA, Williams JS, Brems JJ. Laser capsulorrhaphy for multidirectional instability of the shoulder. An outcome study and proposed classification system. Am J Sports Med. 2003 Jan-Feb;31(1):26-35. [ PubMed ]5.
- Simonet WT, Melton LJ, Cofield RH, Ilstrup DM. Incidence of anterior shoulder dislocation in Olmsted County, Minnesota. Clin Orthop Relat Res. 1984 Jun;(186):186-91. [ PubMed ]6.
- Krøner K, Lind T, Jensen J. The epidemiology of shoulder dislocations. Arch Orthop Trauma Surg. 1989;108(5):288-90. [ PubMed ]7.
- Nordqvist A, Petersson CJ. Incidence and causes of shoulder girdle injuries in an urban population. J Shoulder Elbow Surg. 1995 Mar-Apr;4(2):107-12. [ PubMed ]8.
- Shah A, Judge A, Delmestri A, Edwards K, Arden NK, Prieto-Alhambra D, Holt TA, Pinedo-Villanueva RA, Hopewell S, Lamb SE, Rangan A, Carr AJ, Collins GS, Rees JL. Incidence of shoulder dislocations in the UK, 1995-2015: a population-based cohort study. BMJ Open. 2017 Nov 14;7(11):e016112. [ PMC free article ] [ PubMed ]9.
- Leroux T, Wasserstein D, Veillette C, Khoshbin A, Henry P, Chahal J, Austin P, Mahomed N, Ogilvie-Harris D. Epidemiology of primary anterior shoulder dislocation requiring closed reduction in Ontario, Canada. Am J Sports Med. 2014 Feb;42(2):442-50. [ PubMed ]10.
- Zacchilli MA, Owens BD. Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Joint Surg Am. 2010 Mar;92(3):542-9. [ PubMed ]11.
- Owens BD, Duffey ML, Nelson BJ, DeBerardino TM, Taylor DC, Mountcastle SB. The incidence and characteristics of shoulder instability at the United States Military Academy. Am J Sports Med. 2007 Jul;35(7):1168-73. [ PubMed ]12.
- Kawasaki T, Ota C, Urayama S, Maki N, Nagayama M, Kaketa T, Takazawa Y, Kaneko K. Incidence of and risk factors for traumatic anterior shoulder dislocation: an epidemiologic study in high-school rugby players. J Shoulder Elbow Surg. 2014 Nov;23(11):1624-30. [ PubMed ]13.
- Gibbs DB, Lynch TS, Nuber ED, Nuber GW. Common Shoulder Injuries in American Football Athletes. Curr Sports Med Rep. 2015 Sep-Oct;14(5):413-9. [ PubMed ]14.
- Kraeutler MJ, Currie DW, Kerr ZY, Roos KG, McCarty EC, Comstock RD. Epidemiology of Shoulder Dislocations in High School and Collegiate Athletics in the United States: 2004/2005 Through 2013/2014. Sports Health. 2018 Jan/Feb;10(1):85-91. [ PMC free article ] [ PubMed ]15.
- Kraeutler MJ, McCarty EC, Belk JW, Wolf BR, Hettrich CM, Ortiz SF, MOON Shoulder Instability Group. Bravman JT, Baumgarten KM, Bishop JY, Bollier MJ, Brophy RH, Carey JL, Carpenter JE, Cox CL, Feeley BT, Grant JA, Jones GL, Kuhn JE, Kelly JD, Ma CB, Marx RG, Miller BS, Sennett BJ , Smith MV, Wright RW, Zhang AL. Descriptive Epidemiology of the MOON Shoulder Instability Cohort. Am J Sports Med. 2018 Apr;46(5):1064-1069. [ PubMed ]


















{kind=link}