
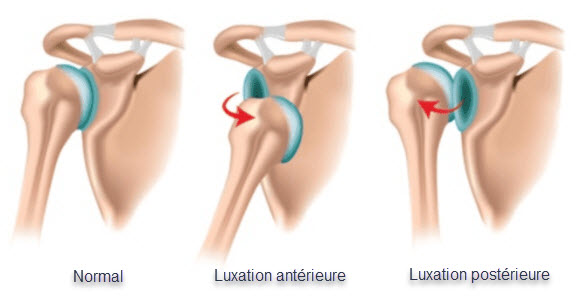
Shoulder instability usually occurs when the shoulder joint lining (capsule), ligaments or labrum are stretched, torn or detached (dislocation), allowing the humeral head to move completely (dislocation) or partially (subluxation) out of the glenoid fossa.
The shoulder is the joint with the most joint movement. In fact, it has few bony limitations in its movements. In the shoulder, this responsibility is transferred to the tissues that envelop it. This arrangement makes the shoulder vulnerable to dislocation and dislocation.
A rim of cartilage called the glenoid bulge surrounds the glenoid fossa. This rim helps the fossa to gain depth, thus helping to prevent dislocation. The most common dislocations are anterior or when the head of the humerus is in abduction and external rotation.
Catégories
1. Traumatic
- Traumatic shoulder instability is a common condition that, especially in younger patients, is associated with high recurrence rates.
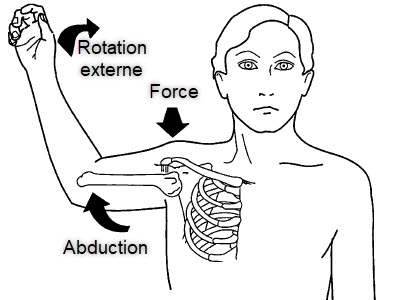
- Anterior dislocation due to trauma is the most common type, 90-95% of cases, usually as a result of sports accidents or falls, especially when the upper extremity is in 90° abduction and external rotation.
- Posterior dislocations are most often the result of seizures, shocks and falls.
2. Non-traumatic
- Congenital instabilities;
- From birth
- Chronic recurrent instability
- After surgery for shoulder dislocation, due to damage to the glenoid rim.
Anterior dislocation of the shoulder
An anterior shoulder dislocation is usually caused by a blow to the abducted, externally rotated and extended arm (for example, blocking a basketball shot). Less commonly, a blow to the posterior humerus or a fall on an outstretched arm can cause an anterior dislocation.
The arm is usually held in an abducted and externally rotated position. There is loss of normal deltoid contour and the acromion is prominent posteriorly and laterally. The humeral head itself may well be palpable anteriorly.
On closer examination, there may be specific damage to the bony, vascular, and nerve structures in the area. It is important to record the neurovascular status before attempting a reduction. In the longer term, rotator cuff damage may also occur.
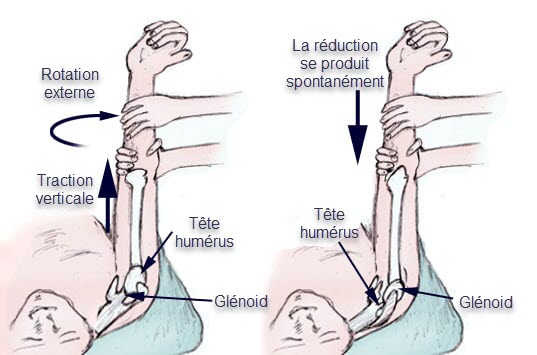
Reduction of anterior shoulder dislocations using the Spaso technique
The Spaso technique is a commonly used technique for the reduction of anterior shoulder dislocation in the injured patient without anesthesia. It consists of forward flexion, external rotation and gentle traction for the reduction of anterior shoulder dislocations with the patient in the supine position (lying on the back).
Symptoms
Symptoms of a dislocated shoulder include:
- Deformation
- Swelling
- Numbness
- Weakness
- Bruising


















{kind=link}