

Snapping scapula syndrome is a dysfunction caused by overuse of the stabilizing muscles of the scapula. A clicking, grinding noise will be felt when moving it on the rib cage. Poor sitting posture with rounded shoulders is often the cause of this syndrome.
Synonym: scapulocostal syndrome, scapulothoracic syndrome
What are the muscles involved in snapping scapula syndrome?
- Levator scapulae
- Pectoralis minor
- Serratus anterior
- Rhomboids
- Infraspinatus and teres minor (less important)
It is a chronic myofascial pain syndrome when the scapo-humeral movement is unbalanced.
Articulation of the scapula
- Scapulocostal: The scapulocostal joint is where the scapula articulates with the posterior rib cage. This is a difficult area to access for trigger point myofascial release. Often, this area is overlooked in therapy by believing the discomfort is on the dorsal surface of the scapula instead of between the scapula and the ribs. It is important to free the scapula by passively bringing it into abduction (do not bring the arm into abduction, but only the scapula by pushing the medial rim laterally). This will help you feel the tension under the scapula better.
- Scapulothoracic : The scapulothoracic junction is a connection between the anterior surface of the scapula and the superolateral surface of the chest wall. The first is slightly concave towards the front, while the second is accordingly convex. The surfaces do not adhere directly to each other.
- Glenohumeral
- Acromioclavicular
Each joint is important and must work with the others, otherwise joint dysfunction will set in, resulting in symptoms that may become chronic and difficult to treat.



Glenohumeral and scapulothoracic movement
- The scapula gives the glenohumeral joint (shoulder) a stable base from which to operate (move).
- The scapula itself slips, slides and spins at a 2: 1 ratio with the shoulder.
- This means that for every two degrees of shoulder movement (flexion or abduction), the scapula moves one degree across the chest wall.
- Scapulothoracic movement requires proper length-to-tension relationships between the scapular bone and all surrounding muscles.
- Any change in the glenohumeral / scapulothoracic ratio can result in impaired or compromised movement of the shoulder.
- This imbalance is called snaping scapula syndrome.
Scapulohumeral breakdown
- Snapping scapula syndrome is characterized by a pop or snap when the arm is raised above the head.
- The term for this sound is crepitus.
- Sound is produced by the friction of the soft tissue between the scapula and the chest wall.
- The tissue stuck between these two structures could be a bursa, a tendon, or a muscle.
- The person with this problem may or may not feel pain when moving.
- There isn’t a reason someone develops snapping scapula syndrome.
- Studies show that sometimes there is a change in the shape or curvature of the scapula.
- After years of movement, the repetitive movement eventually causes a pattern of wear and tear that results in snapping scapula syndrome.
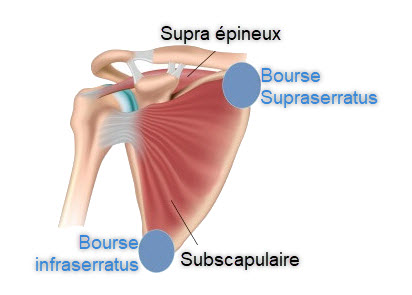
- It is possible that the snap came from supraserratus and infraserratus dung which over time (complex trauma and repair) has become with a very irregular surface. This bursa located between the scapula and the costal surface may become compressed and become weakened if poor posture with rounded shoulders is present.
What are the symptoms of snapping scapula syndrome?
Snapping scapula syndrome is manifested by the insidious development of pain in the upper or posterior aspect of the shoulder girdle with irradiation in one or more of the following regions:
- Neck and occiput, often associated with severe headaches.
- The upper arm, especially in the upper triceps and the point of insertion of the deltoid muscle.
- Around the chest to the front of the chest wall.
- Down the medial aspect of the forearm into the hand and fingers. There is often numbness and tingling in the fingers, most often the fourth and fifth.

























{kind=link}