

Introduction: A deep pain coming from the shoulder
When the shoulder begins to make itself heard, with a dull, poorly localized pain that persists despite rest or conventional care, we readily think of tendonitis, a rotator cuff injury or joint instability. But sometimes, the real culprit is silent, hidden in the twists and turns of the peripheral nervous system: the suprascapular nerve. Still little known outside of specialist circles, this nerve nevertheless plays a central role in the mechanics of the shoulder and can be the cause of chronic pain, loss of strength, or even muscle atrophy if its suffering goes unnoticed.
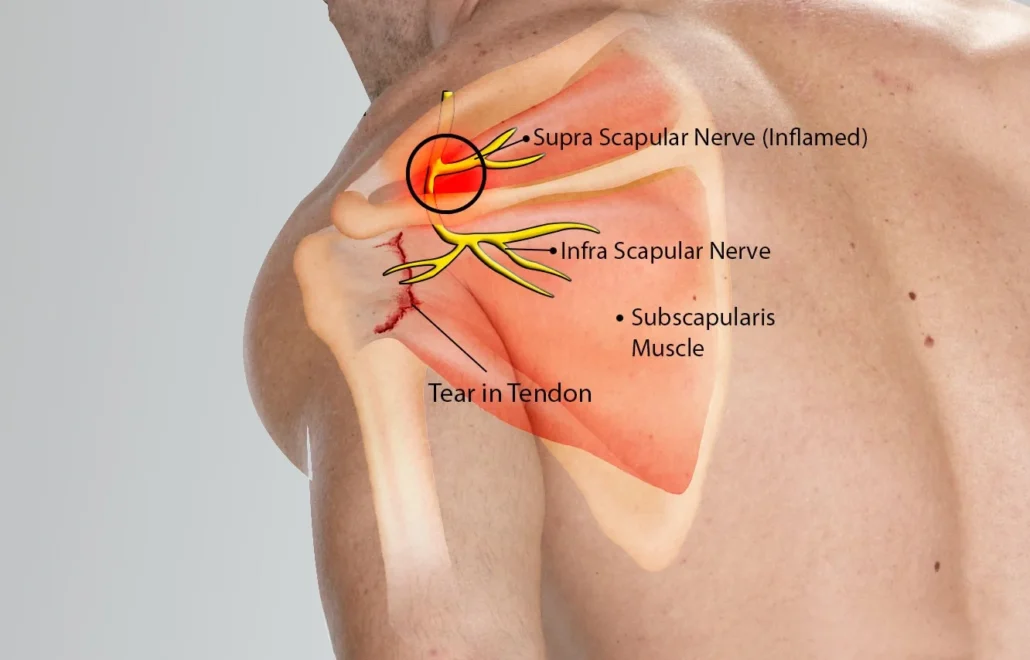
The suprascapular nerve emerges from the C5 and C6 cervical roots of the brachial plexus. It enters narrow anatomical passages, at the level of the scapular notch and then the spinoglenoid notch, to innervate two muscles essential to the dynamic stability of the shoulder: the supraspinatus and the infraspinatus. These two muscles, pillars of the rotator cuff, are involved in the elevation and external rotation of the arm, movements ubiquitous in daily life and in many professional or sporting gestures. Any damage to the suprascapular nerve can therefore lead to a cascade of mechanical and neuromuscular imbalances, progressively worsening functional disorders of the shoulder.
The causes of suprascapular nerve pain are numerous. They range from mechanical compression by a cyst or thickened ligament to repeated traction on the nerve during athletic movements such as throwing, climbing, tennis, or volleyball. Manual workers, musicians, or people with chronic stooped posture can also develop local tension that promotes nerve irritation. This compression syndrome is often insidious, progressive, and poorly diagnosed because its symptoms mimic those of other, more common pathologies: posterior-superior shoulder pain, muscle weakness, stiffness, or even a feeling of blockage.
However, an accurate diagnosis is essential, as treatment varies depending on the nature of the problem: neurological, muscular, articular, or mixed. Medical imaging (MRI, ultrasound) can visualize cysts or signs of muscle atrophy, but the clinical examination remains central. Certain specific tests, such as the resisted external rotation test, combined with a detailed assessment of posture, range of motion, and scapular coordination, can point to suprascapular nerve involvement.
This is where osteopathy comes into its own. Far from being limited to symptomatic treatment, it offers an integrated view of bodily function. The practitioner seeks to understand why this nerve, among many others, has been subjected to excessive stress. Is it chronic upper cervical tension compressing the C5-C6 nerve roots? Poor clavicle mobility altering the tension in the nerve pathway? A diaphragmatic or pelvic dysfunction altering the postural muscle chains up to the scapula? The osteopath does not treat an isolated nerve, but restores the dynamic relationships between structures, releasing areas of conflict, restarting local circulation, and facilitating neuromuscular relaxation.
This comprehensive approach complements functional rehabilitation, particularly to prevent recurrence. An irritated nerve isn’t just tissue that needs to be decompressed; it’s also a messenger that needs to be listened to. It often signals a profound imbalance in the organization of movement and posture. Restoring mobility, releasing myofascial tension, and reharmonizing the body as a whole not only relieves pain, but also prevents chronic pain and compensation elsewhere in the body.
In this article, we’ll explore in detail the anatomy of the suprascapular nerve, the main causes of its lesions, the clinical presentations to recognize, conventional treatments, and most importantly, the specific osteopathic approach that can help restore function, fluidity, and joint comfort. A deep dive into this key structure, often overlooked but essential to intelligent movement.
Anatomy of the suprascapular nerve: a narrow passage with major challenges
The suprascapular nerve is one of the first collateral branches originating from the superior brachial plexus, more precisely from the C5 and C6 nerve roots. Although of modest caliber, its role is far from trivial: it innervates two essential deep muscles of the shoulder – the supraspinatus muscle and the infraspinatus muscle – and indirectly participates in the functional balance of the scapulohumeral joint. Understanding its trajectory, its anatomical relationships and its areas of vulnerability is essential for understanding compression syndromes and their osteopathic management.
Origin and course of the suprascapular nerve
The nerve originates in the upper trunk of the brachial plexus in the neck, between the anterior and middle scalene muscles. It descends laterally and posteriorly, passing under the omohyoid muscle, and then heads toward the scapular notch, a small notch located at the upper part of the scapula. This notch, bridged by the superior transverse ligament, forms a rigid tunnel through which the nerve must pass. This is where the first potential site of compression occurs .
After crossing this notch, the nerve enters the supraspinous fossa , where it gives its motor branches to the supraspinatus muscle, then continues its course towards the spinoglenoid notch. This second notch, more inferior and lateral, is surmounted by the spinoglenoid ligament , and constitutes a second frequent point of compression , particularly in athletes performing repeated movements of abduction and external rotation.
The nerve then reaches the infraspinous fossa , where it innervates the infraspinatus muscle. It can also send out sensory branches to the glenohumeral and acromioclavicular joints, explaining the pain referred to these areas in cases of irritation or neuropathy.
Innervated muscles: discreet but fundamental stabilizers
The muscles innervated by the suprascapular nerve play a fundamental role in the active stability of the shoulder:
- The supraspinatus (or supraspinatus) muscle is located in the supraspinous fossa, above the scapular spine. It participates in the initial abduction of the arm (the first 15° before the deltoid takes over), but above all, it acts as a dynamic coaptor of the humeral head against the glenoid cavity.
- The infraspinatus , located under the spine of the scapula, is one of the main external rotators of the arm. It acts in synergy with the teres minor and stabilizes the humeral head during rotation and elevation movements.
Nerve damage results in hypotonia or atrophy of these muscles, unbalancing the rotator cuff, promoting subacromial impingements and secondary tendinopathies.
Critical passage zones: anatomical traps
The bony configuration of the scapula, the ligaments that bridge the notches, and the local biomechanical constraints make the suprascapular nerve a vulnerable candidate for compression . These can occur in two specific areas:
- The superior scapular notch , especially when the superior transverse ligament is ossified or thickened. This situation can be congenital or related to repeated microtraumas.
- The spinoglenoid notch , often involved in throwing or racquet sports athletes, due to dynamic stretching or compression related to movement.
It is important to note that the nerve passes under the ligaments , while the corresponding arteries and veins surmount them. This arrangement explains why some vascular disorders are not associated with neuropathy, and vice versa.
Relations with neighboring structures
The path of the suprascapular nerve crosses or runs alongside several osteopathically relevant structures:
- The middle scalene muscle , whose tensions can influence the dynamics of the brachial plexus.
- The clavicle , particularly its tilting and rotating movements during shoulder movements.
- The coracoid ligament and the coracoid process , close to the vascular-nervous pathways.
- The cervicothoracic fascia , which transmits deep postural tensions to the scapula.
A rigorous osteopathic approach will seek to assess all of these interfaces to relieve areas of mechanical stress that may affect the nerve.
Causes of suprascapular nerve injuries: between compression, tension and global imbalances
The suprascapular nerve, although buried deep within the scapula, is subject to numerous constraints that can compromise its function. Its winding path through narrow bony passages, its proximity to rigid ligamentous structures, and its involvement in precise technical movements make it particularly vulnerable. The lesions that affect it are mainly mechanical , but can also be part of a postural, traumatic, or degenerative context , which the osteopath must take into account as a whole.
Compression in the scapular notch: the superior transverse ligament trap
One of the most common causes of suprascapular neuropathy is compression in the scapular notch , where the nerve passes under the superior transverse ligament . This ligament may be thickened , ossified , or simply tense , reducing the diameter of the nerve’s passage. This type of compression is often silent at first, then gradually becomes symptomatic as myelin is impaired and nerve conduction slows.
This situation is frequently encountered in:
- throwing athletes ( baseball, javelin),
- the climbers ,
- tennis or volleyball players ,
- but also elderly people with degenerative changes or ligament calcifications.
In these cases, the osteopath will focus on cervical tension , clavicle mobility , scapular dynamics , and cervicothoracic fascia which can indirectly influence this narrow passage area.
Compression in the spinoglenoid notch: the vulnerability of the moving nerve
The second possible site of compression is the spinoglenoid notch , located between the scapular spine and the glenoid cavity. Here, the nerve passes under the spinoglenoid ligament , just before joining the infraspinatus muscle. This passage is particularly sensitive to tensile forces , especially in external rotation and arm elevation movements.
High-velocity or repetitive movements , combined with forced external rotation (such as serving in tennis or smashing in volleyball), can lead to chronic microtraction of the nerve , promoting perineural inflammation and then secondary compression.
Para-articular cysts or synovial cysts , often resulting from lesions of the glenoid labrum, can also lodge in this area and exert pressure on the nerve. These formations can be revealed by MRI, but their mechanical origin should make the osteopath think: why did such excess joint pressure generate synovial leakage in this area?
Repetitive gestures, microtraumas and functional overload
Even without any anatomical narrowing or visible injury, the suprascapular nerve can be irritated by functional overload . This concerns:
- manual workers ( mechanics, painters, hairdressers);
- musicians , whose prolonged static posture in external rotation can lead to continuous tension;
- sedentary people adopting a prolonged hunched posture, with a scapula fixed in downward rotation.
In these cases, the nerve is subjected to constant adaptive tension . It is not strangled, but pulled , stretched , irritated by the loss of mobility of its environment. This type of injury is insidious, often invisible to imaging , but very real in the patient’s experience.
The osteopathic approach will then focus on a global decompression of the peripheral nervous system: relaxation of postural chains, scapular reharmonization, release of cervico-dorsal tensions and restoration of micro-movements of the scapula on the costal grill.
Traumatic and iatrogenic causes
Direct trauma to the scapula (falls, fractures, acromioclavicular or glenohumeral dislocations) can damage the nerve by:
- sudden pull ,
- compressive hematoma ,
- excessive stretching during a subluxation.
Furthermore, certain surgical procedures (rotational cuff repair, shoulder stabilization, cyst excision) can cause accidental injury or postoperative fibrosis around the nerve.
In these cases, osteopathy will often intervene in the post-acute phase , to restore local trophicity, promote tissue decompression, and support neuro-motor plasticity.
Postural integration and global enabling factors
Finally, certain morphologies or chronic adaptations can promote suffering of the suprascapular nerve:
- Thoracic hyperkyphosis : closing the scapulocostal space.
- Scoliosis or thoracic rotation : altering the support of the scapula.
- Diaphragm dysfunctions : altering breathing and posture.
- High costal fixations : resulting in loss of scapular glide.
These elements, often overlooked, are essential to correct to ensure lasting healing.
Symptoms and differential diagnosis: deciphering an often misunderstood pain
Suprascapular nerve injuries present a clinical picture that is both specific and confusing. They are often underdiagnosed because their symptoms mimic other common shoulder pathologies, such as rotator cuff tendinopathies or subacromial impingements. The role of the osteopath – and of any clinician – is therefore to distinguish the warning signs , to question the context, and to integrate a careful listening of the body as a whole. Because if the nerve speaks, it is sometimes through indirect channels.
Pain: localized, persistent, often posterior-superior
The most common symptom is a deep pain behind and above the shoulder, in the posterior-superior scapular region. It is often poorly localized , described as a dull, heavy discomfort, sometimes radiating to the neck or arm. It can occur:
- at rest , especially if the compression is constant;
- during movements , particularly in abduction or external rotation;
- after an effort , reflecting cumulative mechanical suffering.
In some cases, pain is absent , but it is the loss of strength or rapid muscle fatigue that becomes the warning sign.
Muscle weakness and atrophy: signs of prolonged damage
When nerve compression is prolonged, the muscles it innervates – supraspinatus and infraspinatus – gradually lose their trophicity. This atrophy is observable:
- on palpation (digging above or below the spine of the scapula);
- to active mobilization (loss of strength in abduction or external rotation);
- to visual observation (scapular muscle asymmetry).
This motor deficit is often compensated by other muscles (deltoid, upper trapezius), which can induce poor motor patterns and create secondary pain, particularly cervical or scapular.
Altered shoulder function
The patient frequently reports difficulty raising the arm above the horizontal, a feeling of weakness , or a loss of precision in fine movements. In athletes, this manifests itself as a drop in performance: loss of speed when throwing, imprecision, pain at the end of the movement.
The resisted external rotation test is often positive, as are the supraspinatus muscle fatigue tests (resisted straight arm raise), which reveal a rapid drop in strength.
Osteopathic clinical examination: beyond orthopedic tests
The role of the osteopath is fundamental here, because beyond specific tests, he will explore:
- scapulothoracic dynamics : sliding, mobility, scapulohumeral rhythm;
- cervical tensions ( C4 to C7), particularly the C5 and C6 roots;
- costal and diaphragmatic mobility , often restricted in chronic cases;
- the fascial quality of the axilla, posterior thorax and neck.
These elements make it possible to reconstruct a map of the tensions which explain the suffering of the nerve, even in the absence of visible lesion on imaging.
Contributions of medical imaging
- MRI is the reference examination: it allows visualization of a possible para-articular cyst , muscular atrophy , or ligament thickening .
- Ultrasound can also be useful in detecting atrophy or dynamic abnormality during movement.
- Electromyography (EMG) can confirm suprascapular nerve neuropathy, by demonstrating slowed conduction or partial denervation.
However, it is important to note that imaging can sometimes be normal , particularly in cases of functional nerve damage without visible anatomical lesion. In these situations, tissue listening and osteopathic perception take on their full meaning.
Differential diagnosis: do not confuse shoulder pain
The symptomatology of the suprascapular nerve can mimic or coexist with several pathologies:
- Supraspinatus tendinopathy : similar pain but without atrophy.
- Subacromial impingement : pain when raising the arm, often mechanical.
- Acromioclavicular arthropathy : more anterior pain.
- Thoracic outlet syndrome : irradiation into the arm, paresthesia, more diffuse symptoms.
- Cervical osteoarthritis C5-C6 : referred pain, but often associated with radicular signs.
The differential diagnosis is based on a rigorous clinical approach , integrating the patient’s history, palpatory examination, functional tests and, if necessary, additional examinations.
Medical and rehabilitation treatments: relieve, restore, prevent
Once a diagnosis of suprascapular nerve neuropathy has been made or is strongly suspected, conventional management is based on three pillars: relieving inflammation , restoring muscle function , and preventing recurrence . The approach is often multidisciplinary, combining medicine, physiotherapy, and increasingly, manual interventions such as osteopathy . In this section, we explore conventional therapeutic strategies before putting their complementarity with osteopathic care into perspective.
Relative rest and modification of aggravating gestures
In the acute phase, the objective is to limit mechanical stress on the nerve . It is generally recommended:
- Temporary cessation of sporting or professional activities involving repetitive abduction or external rotation movements ;
- Adapting working and resting posture (avoiding sleeping on the affected side, correcting shoulder rolling);
- Wearing a brace or taping to stabilize the scapula and reduce excessive traction on the nerve.
This rest is relative : it is not a question of totally immobilizing the shoulder, but of avoiding excessive loads while maintaining gentle functional mobility , to avoid secondary stiffness.
Drug treatment: anti-inflammatories and infiltration
When pain is significant, nonsteroidal anti-inflammatory drugs (NSAIDs) are often prescribed to reduce local inflammation. Their effectiveness varies, but they can provide temporary relief , making it easier to begin rehabilitation.
In the event of confirmed compression (particularly due to a cyst or ligamentous conflict), a corticosteroid injection may be proposed. It is carried out:
- either in the supraspinous fossa , under ultrasound guidance;
- or near the spinoglenoid notch.
This infiltration has a dual role: anti-inflammatory and diagnostic (the temporary disappearance of pain after the injection confirms the involvement of the nerve). However, repeated infiltrations can have side effects, including weakening of the tissues or local demineralization , hence the importance of a cautious and reasoned approach.
Functional rehabilitation: restoring movement, not just muscle
Rehabilitation is a central part of recovery. It aims not only to strengthen deficient muscles , but also to re-educate the overall movement of the shoulder , working on the coordination between the scapula, the clavicle, and the humerus.
Key steps include:
- Progressive strengthening of the supraspinatus and infraspinatus, particularly in moderate and painless ranges of motion;
- Scapular stabilization , by activating the fixators (anterior serratus, middle and lower trapezius) to restore freedom to the scapula;
- Proprioceptive work , to restore the quality of movement and prevent overcompensation;
- Assisted active mobility , to combat stiffness and maintain joint range of motion.
Physical therapists sometimes use techniques such as electrical stimulation, biofeedback, or closed-chain exercises to strengthen motor engagement without excessive overload.
Surgical treatment: a rare but sometimes necessary option
In some cases, when nerve compression is clearly demonstrated and resists conservative treatment for several months, surgical decompression may be considered. It consists of:
- release the nerve at the level of the scapular or spinoglenoid notch;
- remove a compressive cyst ;
- or sever a thickened ligament.
Surgery is usually performed arthroscopically, with relatively rapid functional recovery. However, the prognosis depends largely on the duration of symptoms : the longer the condition has been present, the higher the risk of irreversible atrophy.
The contribution of therapeutic education
Finally, an often overlooked but fundamental aspect is patient education :
- understanding of its anatomy and pathology;
- correction of daily gestures;
- autonomy in maintenance exercises;
- load management (progressiveness, recovery, postural hygiene).
This educational work, in which the osteopath can play a major role, allows the patient to be actively involved in their recovery and to prevent relapses, especially among athletes or exposed professionals.
The osteopathic approach: restoring neuro-mechanical balance
In the treatment of peripheral neuropathies such as that of the suprascapular nerve, osteopathy finds a privileged field of expression . Not to directly “repair” the injured nerve, but to reduce mechanical constraints , rebalance the myofascial chains , and promote an optimal tissue environment for neuromuscular recovery. Far from a segmental or symptomatic approach, the osteopath engages in a global reading of the body: why is this nerve suffering? What old or recent tensions have converged towards this area? And above all, how can we restore a coherent, fluid freedom of movement , respectful of natural compensation mechanisms?
A comprehensive osteopathic diagnosis: beyond the painful shoulder
The osteopathic assessment of a patient with suprascapular nerve injury does not stop at the shoulder. It includes:
- A complete postural analysis : asymmetries, scoliotic posture, rolling of the upper thorax, anterior projection of the shoulders;
- Palpation of fascial tension in the neck, thorax, scapular region and diaphragm;
- A detailed assessment of joint mobility : clavicle, scapula, ribs, cervical-dorsal spine, thoracolumbar hinge, pelvis;
- Identification of areas of loss of mobility , restriction of tissue sliding , or viscerosomatic fixation , which may disrupt the innervation, vascularization or lymphatic drainage of the region concerned.
This global diagnosis makes it possible to determine whether the suprascapular neuropathy is primary (traumatic, compressive) or secondary to deeper imbalances , which should be treated as a priority.
Release of compression areas: cervical, clavicle, scapula
Three anatomical areas are often involved in the genesis or maintenance of suprascapular nerve compression:
- The upper and middle cervical spine (C4 to C6), whose vertebral dysfunctions can disrupt the emergence of the upper trunk of the brachial plexus, from which the nerve arises;
- The clavicle , particularly in its posterior rotation and elevation movements, which influence ligament tensions around the scapular notch;
- The scapula , whose loss of mobility or myofascial adhesions (infraspinatus, latissimus dorsi, trapezius) can disrupt the gliding of the nerve in its anatomical passages.
Osteopathic techniques used include:
- Gentle joint mobilizations (clavicle, AC, SC, scapulocostal);
- Targeted cervical decompression ;
- Deep fascial normalizations around the supra- and infraspinous fossa;
- Myotensive techniques on hypertonic muscles (upper trapezius, levator scapula, rhomboids) which contribute to mechanical compression.
Work on the myofascial chains and diaphragm: the remote link
The suprascapular nerve is not only influenced locally. It is integrated into broader postural functional chains. Thus:
- Diaphragm dysfunction can alter intrathoracic pressure, disrupt scapular posture, and promote upper thoracic rolling;
- High rib fixation ( 1st to 3rd rib) can reduce the freedom of the scapula, leading to continued tension in the upper scapular region;
- Lumbar or pelvic compensations ( iliac tilt, sacroiliac block) can create ascending chains of tension.
Osteopathic treatment will therefore include remote techniques, aimed at:
- Release the thoracolumbar hinge (role in the transmission of respiratory pressures);
- Reharmonize the postural cross chains ;
- Restore mobility to the diaphragm and abdominal fascia, to restore ample and fluid breathing, essential for scapulothoracic balance.
Restart microcirculation and neuro-tissue drainage
A compressed nerve is a nerve whose vascularization is altered . Osteopathic work also aims to:
- Improve local venous and lymphatic circulation ;
- Facilitate the drainage of pro-inflammatory toxins;
- Reduce congestion of soft tissue around the nerve pathway.
Gentle circulatory stimulation techniques, tissue stretching, or visceral mobilization (liver, renal region) can indirectly improve the metabolic environment of the nerve.
Somato-emotional integration: the memory of the irritated nerve
In chronic cases, or when the pain is disproportionate to the visible lesions, the osteopath can explore the somato-emotional dimension . The nerve, irritated for a long time, can maintain a sensory imprint , a memory of pain or vulnerability, which maintains the suffering beyond the tissue signal.
More subtle approaches, such as:
- the craniosacral (regulation of the autonomic nervous system),
- work on neurotissue rhythm ,
- or deep tissue listening (biodynamic approach),
can help release deep, often unconscious resistance.
Prevention and practical advice: protecting the nerve on a daily basis
Once the pain has been relieved and function has been partially or completely restored, preventing recurrence becomes a fundamental issue. The suprascapular nerve, due to its enclosed anatomy and its function in complex shoulder movements, remains vulnerable to any sudden, unbalanced or poorly adapted resumption of activity . Whether you are an athlete, manual worker, musician or sedentary, certain simple adjustments in lifestyle, posture and movement can help preserve neuromuscular balance and prevent the return of pain.
Optimizing professional and sporting gestures
One of the major factors in suprascapular nerve overload is the excessive repetition of abduction and external rotation movements . These movements intensely stress the muscles innervated by the nerve (supraspinatus and infraspinatus) and can lead to cumulative microtrauma.
Practical recommendations:
- Reduce extreme range of motion without warming up, especially movements above the shoulder;
- Adjust the height of work surfaces to avoid prolonged postures with arms raised (hairdressers, painters, electricians, etc.);
- Incorporate active breaks every 30 to 45 minutes of work or training;
- For athletes, insist on a complete warm-up of the shoulder , including scapular mobility, the rotator cuff and the posterior chain.
In osteopathy, we can also work before resuming an activity to prepare the body , lift residual joint restrictions, and prevent a repetitive movement from triggering a silent compression.
Strengthen the rotator cuff and stabilizer muscles
A damaged nerve makes the muscles it innervates less efficient. It is therefore essential to strengthen the rotator cuff muscles , but also the stabilizing muscles of the scapula (serratus anterior, lower trapezius, rhomboids) in order to relieve mechanical stress.
Simple preventive exercises:
- Lateral raises in external rotation with elastic or light weight, elbow flexed at 90°;
- Rowing in a prone position , to activate the lower trapezius;
- Wall slide movements , along a wall, to promote scapulohumeral coordination;
- Scapular sheathing in facial support, controlling the stability of the scapula.
These exercises should be performed slowly , painlessly, with an emphasis on the quality of movement rather than the load. The osteopath can guide the patient to a physiotherapist or qualified trainer to establish a personalized program.
Promote a dynamic posture on a daily basis
Posture plays a central role in the health of the suprascapular nerve. Exaggerated thoracic kyphosis , rolled shoulders , or chronic scapular immobility can create ongoing tension on the nerve, even in the absence of repetitive movement.
Osteopathic tips for healthy posture:
- Do not seek the “correct fixed posture” but favor frequent movement (alternating between sitting and standing, regular walking);
- Use lumbar support or a dynamic seat if you work long hours sitting down;
- Regularly relax the cervical-dorsal muscles (trapezius, levator scapulae) through self-stretching or self-massage with a ball or roller;
- Work on diaphragmatic breathing , to restore fluid costal dynamics and prevent upper thoracic rolling.
The osteopath can suggest postural integration exercises , linked to proprioception and movement coordination, adapted to the patient’s profile.
Integrate breath and fluidity into movement
Breathing is an often overlooked pillar of prevention. A fixed diaphragm, high thoracic breathing, or inhibition of the respiratory rhythm can contribute to an alteration of the scapulothoracic rhythm .
Respiratory recommendations:
- Practice cardiac coherence or slow breathing exercises (6 breaths/min) to soothe the autonomic nervous system;
- Mobilize the upper ribs by stretching while inhaling maximum (hands on the upper thorax, opening in a cross);
- Combine movement and breath in each exercise: inhale when opening, exhale during the effort.
Breathing then becomes a therapeutic ally, but also a revealer of deep tensions. The osteopath can guide his patient in this reconnection to the body through breathing , promoting the release of chronic tensions around the shoulder blade.
Conclusion: listen to the nerve, hear the deep imbalance
Suprascapular nerve pain is often subtle, insidious, hidden behind common shoulder pain or postural compensations. And yet, it reflects much more than a simple mechanical conflict: it reveals an imbalance in the subtle coordination of movement , a loss of fluidity in everyday gestures , a silent over-solicitation that ends up breaking the harmony.
The osteopathic approach, by freeing itself from the limits of the local and the visible, makes it possible to link causes to consequences , to re-establish tissue respiration where compression, tension or inflammation had set in. It does not oppose medical care to rehabilitation, but complements them, by offering the body a space for relaxation, self-repair, and above all functional reintegration .
Treating the suprascapular nerve is not just about freeing a narrow passage. It is about restoring the dialogue between the neck, thorax, shoulder, and pelvis. It is about reintegrating the arm into the entire posture, and the posture into an embodied experience of movement that is conscious, flexible, and adaptive.
Every chronic pain is an invitation to readjust, to slow down, to feel. The nerve, far from being a simple guiding thread, becomes a precious messenger , an entry point towards a finer understanding of our internal balance. It is still necessary to listen to it accurately, and accompany it with respect.
References
- Mallon WJ, Dutcher JP. “Suprascapular nerve: normal anatomy and pathologic findings on MRI” , AJR Am J Roentgenol. 2006;186(2):367-372.
➤ Review of suprascapular nerve anatomy and compression points on MRI. - Boykin RE, Friedman DJ, Higgins LD, Ponce BA, Warren RF, Warner JJP. “Suprascapular neuropathy” , J Bone Joint Surg Am. 2010;92(13):2348-2364.
➤ Comprehensive analysis of the causes, diagnoses, and treatments of suprascapular neuropathies. - Martin SD, Warren RF. “Current concepts review: suprascapular neuropathy” , J Bone Joint Surg Am. 1997;79(3):463–470.
➤ One of the seminal articles on the understanding of nerve compression syndromes. - Lafosse L, Tomasi A, Corbett S, Baier GP, Willems K. “Arthroscopic release of suprascapular nerve entrapment at the suprascapular notch” , Arthroscopy. 2007;23(6):691.e1–e3.
➤ Description of the surgical technique for arthroscopic nerve release. - Saha S, Gopalkrishna V. “Clinical and surgical anatomy of the suprascapular nerve for neuromuscular interventions” , Clin Anat. 2021;34(6):846–856.
➤ Recent article on the surgical anatomy of the nerve and its therapeutic implications.
References in physiotherapy and rehabilitation
- Anderson MW, Read WM. “Shoulder pain and weakness in the overhead athlete: suprascapular neuropathy” , Curr Sports Med Rep. 2007;6(6):301-307.
➤ Link between sport, repetitive movements and nerve damage. - Kibler WB, McMullen J. “Scapular dyskinesis and its relation to shoulder pain” , J Am Acad Orthop Surg. 2003;11(2):142–151.
➤ Importance of scapular control in the prevention of shoulder pain.
Osteopathic and biomechanical references
- Franke H, Fryer G, Ostelo RWJG, Kamper SJ. “Musculoskeletal manual therapy for patients with radiculopathy” , Cochrane Database Syst Rev. 2015.
➤ Synthesis of evidence on the effects of manual techniques in peripheral neuropathies. - Gleditsch J. “Manual treatment of peripheral nerves” , Éditions Sully, 2008.
➤ Fine osteopathic approach to the peripheral nervous system, including the suprascapular nerve. - Barral JP, Croibier A. “Manual Therapy for the Peripheral Nerves” , Churchill Livingstone Elsevier, 2007.
➤ Essential reference on osteopathic nerve normalization techniques. - Bordoni B, Zanier E. “Clinical and osteopathic considerations in the respiratory diaphragm dysfunction” , Int J Chron Obstruct Pulmon Dis. 2013;8:369–375.
➤ Influence of the diaphragm on posture, scapular tension and peripheral neurological disorders.















{kind=link}