
 (1)")
Introduction
Vertebrobasilar insufficiency (VBI) is a serious condition characterized by impaired blood flow to the posterior regions of the brain, including the brainstem, cerebellum, and occipital lobes. This condition can be due to a variety of causes, such as atherosclerosis, arterial dissection, or external compression of the vertebral arteries, which can lead to a range of symptoms ranging from dizziness and vertigo to severe neurological deficits and stroke-like episodes. Understanding the complex anatomy of the vertebrobasilar system and its susceptibility to various pathologies is essential for the effective management and treatment of VBI.
In the field of therapeutic interventions, cervical manipulation is often used to treat neck pain, headaches, and other musculoskeletal disorders. This technique involves applying specific forces to the cervical spine with the aim of improving joint function, relieving pain, and improving overall mobility. Despite its potential benefits, cervical manipulation has been scrutinized for its possible implications on the vertebrobasilar system, particularly in individuals who may be predisposed to or already have VBI.
The interaction between cervical manipulation and vertebrobasilar insufficiency raises important questions about patient safety and treatment efficacy. On the one hand, cervical manipulation can provide significant relief of musculoskeletal symptoms; on the other hand, it carries the risk of exacerbating or triggering adverse events in patients with compromised vertebrobasilar circulation. It therefore becomes crucial to understand the potential risks associated with cervical manipulation in this setting, as well as to implement evidence-based guidelines to mitigate these risks.
This discussion aims to explore the complex relationship between vertebrobasilar insufficiency and cervical manipulation. By examining the underlying mechanisms of vertebrobasilar insufficiency, the effects of cervical manipulation on the vertebrobasilar system, and current safety protocols, we aim to provide a comprehensive overview that will help healthcare professionals make informed decisions and improve patient safety.
Anatomy of vertebrobasilar insufficiency
Vertebrobasilar insufficiency (VBI) refers to reduced blood flow to the posterior part of the brain, primarily supplied by the vertebral and basilar arteries. These arteries are an integral part of the cerebral circulation, providing approximately 11% of cerebral blood flow, while the remaining 89% is supplied by the carotid system (Grant, 1994a). Understanding the anatomy and biomechanics of the vertebrobasilar system is essential to understand how cervical movements can influence blood flow and potentially lead to insufficiency.
Anatomy of the vertebral arteries
The cervical region is distinguished from other vertebral segments by the presence of vertebral arteries. These arteries arise from the subclavian artery and ascend the cervical spine, entering the transverse foramen of each cervical vertebra from C6. This anatomical pathway is crucial because it exposes the vertebral arteries to potential mechanical stress during cervical movements.
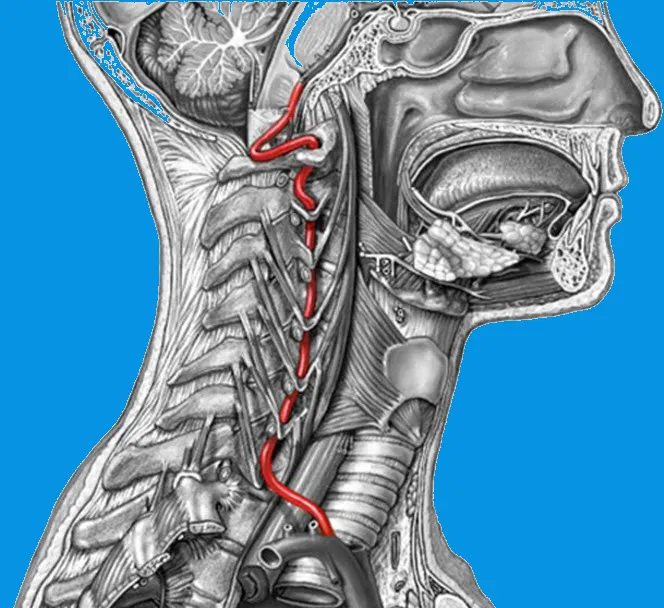
This detailed illustration highlights the complex anatomy of the vertebral artery and its path through the cervical spine and skull base. The vertebral artery, shown in red, is a critical structure that supplies oxygenated blood to the posterior regions of the brain, including the brainstem, cerebellum, and occipital lobes.
Course of the vertebral artery:
- Origin : The vertebral artery arises from the subclavian artery on either side of the body.
- Cervical course : It ascends through the transverse foramina of the cervical vertebrae, from C6 to C1. These openings in the transverse processes protect the artery, but also make its course vulnerable to excessive mechanical forces, such as during sudden movements or trauma.
- Cranial inlet : The artery then passes into the foramen magnum, where it joins the opposite vertebral artery to form the basilar artery, a key structure in the vertebrobasilar circulation.
Clinical significance:
This structure is particularly vulnerable to injury during cervical manipulation or cervical trauma. Dissection of the vertebral artery can lead to decreased blood flow, causing serious neurological symptoms, such as dizziness, visual disturbances, or a cerebrobasilar stroke. This image therefore highlights the importance of a thorough knowledge of anatomy to avoid complications during manual therapeutic interventions.
During their ascent, the vertebral arteries pass through the transverse foramina of the cervical vertebrae. Upon reaching the atlas (C1), the arteries run almost horizontally. They then cross the foramen magnum and join their contralateral counterpart to form the basilar artery, which continues to supply the brainstem, cerebellum, and occipital lobes.
Biomechanics and Blood Flow Considerations
The unique anatomy of the cervical spine means that the vertebral arteries are closely associated with the bony structures of the cervical vertebrae, particularly at the C1 and C2 levels. This anatomical relationship is important during head rotation and other cervical movements. Approximately 45 to 50 degrees of cervical rotation occurs primarily at the atlantoaxial joint, which is essential for allowing a range of head and neck movements.
During rotational movements, the vertebral arteries, attached to the transverse foramina of C1 and C2, are subjected to stretching, tension, compression, and torsion forces. These forces can have a significant impact on blood flow in these arteries. Rotational movement of the head may cause the greatest decrease in blood flow to the vertebral arteries, as shown in several studies (deKleyn and Nieuwenhuyse, 1927; deKleyn and Versteegh, 1933; Tatlow and Bammer, 1957; Toole and Tucker, 1960; Brown and Tatlow, 1963; Andersson et al., 1970; Barton and Margolis, 1975; Grossman and Davies, 1982; Yang et al., 1985). These studies demonstrate that mechanical stress applied during head rotation can result in temporary or persistent reductions in blood flow, contributing to the symptoms of vertebrobasilar insufficiency.
Clinical implications
The anatomy and biomechanics of the vertebrobasilar system highlight the delicate balance required in cervical movements, particularly when interventions such as cervical manipulation are considered. Because the vertebral arteries are sensitive to mechanical stress during cervical rotation, it is essential to be aware of the potential risks associated with these movements, particularly in individuals with compromised vertebrobasilar circulation.
In summary, the unique anatomical course of the vertebral arteries in the cervical spine and their sensitivity to mechanical forces during cervical rotation underscore the importance of careful assessment and management of patients with symptoms related to vertebrobasilar insufficiency. Understanding these anatomical and biomechanical principles helps clinicians make informed decisions regarding treatment options and strategies to minimize risks while optimizing patient care.
Incidence of vertebrobasilar stroke after manual spinal manipulation
Statistics and epidemiological data on vertebrobasilar insufficiency (VBI)
Vertebrobasilar insufficiency (VBI) is a serious condition resulting from a temporary reduction or interruption of blood flow in the vertebrobasilar system, which supplies the posterior regions of the brain. VBI can cause a variety of manifestations, ranging from mild vertigo to major stroke, and its association with cervical manipulation raises important safety concerns. This section explores available statistics and epidemiological data, including the prevalence of VBI, complications related to cervical manipulation, and populations at greatest risk.
1. Prevalence of IVB in the general population
The exact prevalence of IVB in the general population is difficult to determine due to the variability of diagnostic criteria and the lack of specific epidemiological data. However, some studies provide indications of its frequency:
- Vertebrobasilar transient ischemic attacks (TIAs) : TIAs affecting the posterior circulation account for approximately 20% of all TIAs. This proportion suggests that IVB, as an underlying cause, may affect a significant fraction of patients with TIAs.
- Vertebrobasilar Strokes (VBTC) : Strokes involving the posterior circulation constitute approximately 20% of all ischemic strokes. Although not all are directly attributable to a VBTC, this statistic underscores the importance of the vertebrobasilar circulation in cerebral ischemic events.
2. Risk factors for IVB
Certain populations are at increased risk of developing IVB:
- Age : People over 65 are more often affected due to atherosclerosis and decreased elasticity of the vertebral arteries.
- Associated pathologies :
- Atherosclerosis: Main cause in 50% of IVB cases.
- High blood pressure and diabetes: Risk multipliers.
- Cervical trauma : A history of trauma, such as whiplash or repetitive strain injuries, increases the vulnerability of the vertebral arteries.
3. Cervical manipulations and IVB
Cervical manipulation is frequently associated with an increased risk of IVB due to its potential to cause arterial dissections. Available data show a low but significant prevalence:
- Estimated incidence :
- A literature review published in the Journal of Neurology indicates that the risk of spinal dissection after cervical manipulation is estimated at between 1 in 10,000 and 1 in 100,000 sessions. However, these figures vary depending on the populations studied.
- Approximately 25% of vertebral artery dissections are associated with cervical manipulation in some case studies. (Source: Stroke Journal)
- Complications graves :
- A vertebral dissection can lead to a vertebrobasilar stroke in about 1 in 20 cases. These strokes are particularly serious, with a mortality or significant disability rate of up to 30%. (Source: Lancet Neurology)
4. Profiles of patients affected by post-cervical manipulation complications
Epidemiological studies show that complications related to cervical manipulation are more frequent in certain subgroups:
- Age and gender : Young adults, especially women between the ages of 20 and 45, are more vulnerable to arterial dissections. This may be due to differences in arterial wall structure and hormonal changes.
- Absence of prior pathologies : Post-manipulation arterial dissections often occur in young individuals without identifiable vascular risk factors.
5. Comparison with other causes of spinal dissection
Cervical manipulation is just one cause of vertebral artery dissection:
- Spontaneous dissections : These represent 40% of cases of vertebral dissection and are often associated with physical exertion or sudden movements of the neck (for example, sports stretching or violent sneezing).
- Minor trauma : About 35% of dissections are related to minor trauma, such as low-impact car accidents or falls.
6. Specific studies on cervical manipulations and vascular complications
1. Canadian study by Cassidy (2008) :
The key study you are referring to is Cassidy et al., published in 2008 in the journal Spine . This study examined the association between chiropractic care (including cervical manipulation) and the risk of vertebrobasilar (VBAS) stroke. Here are the key findings:
Main results:
- Similar risk : The risk of stroke after cervical manipulation was found to be comparable to that observed during medical consultations for neck pain or headaches.
- Probable trigger : The initial symptoms of an arterial dissection (headache and neck pain) could explain these consultations, suggesting that the underlying pathology was already present before the manipulation.
This study is important because it highlighted that cervical manipulation did not appear to significantly increase the risk of vertebrobasilar stroke when compared to primary medical care.
Reference and link to the study:
- Titre de l’étude : Risk of Vertebrobasilar Stroke and Chiropractic Care: Results of a Population-Based Case-Control and Case-Crossover Study
- Link : Access the full study on Spine
This resource provides an in-depth analysis and is based on rigorous methodology, making it a reliable reference for discussing the link between cervical manipulation and stroke.
2. BMJ Systematic Review (2012) :
In 2012, the British Medical Journal (BMJ) published a debate on whether to abandon cervical manipulation for the treatment of mechanical neck pain. In this exchange, Benedict M. Wand and colleagues argued for abandoning this practice, highlighting the potential risks of serious neurovascular complications, including vertebral artery dissections that can lead to vertebrobasilar strokes. They emphasized that cervical manipulation, although commonly used, has not demonstrated significant superiority over other less risky treatments, calling into question its necessity and prudence in clinical practice.
In response, J. David Cassidy and colleagues defended cervical manipulation, stating that it is a valuable treatment option for patients with neck pain. They cited studies and systematic reviews indicating that cervical manipulation is effective and that the associated risks are low. They also noted that an international multidisciplinary working group recently endorsed manipulation as a first-line treatment for neck pain, whiplash, and associated headaches, based on a systematic review of randomized clinical trials and research on adverse events.
This debate highlights the ongoing controversy regarding the use of cervical manipulation in the treatment of mechanical neck pain. It highlights the need for careful risk-benefit assessment, as well as the importance of considering less invasive treatment alternatives when appropriate.
For a full reading of the arguments presented, you can consult the original BMJ articles via the following links:
7. Relative risk of cervical manipulations compared to medical interventions
Compared to other medical procedures, the risk of serious complications from cervical manipulation remains low but not negligible:
- Risk of stroke following spinal dissection :
- Estimated at 0.002% by cervical manipulation. (Source: Neurology Journal)
- In comparison, the risk of post-traumatic arterial dissection after a car accident is about 10 times higher.
- Perceived versus actual risk :
- A qualitative study showed that patients often associate cervical manipulation with high risk, although the absolute risk remains low. This highlights the importance of risk communication before any procedure.
8. Issues for clinical practice
Epidemiological data demonstrate that although the risk is low, the consequences of a vascular complication after cervical manipulation can be severe. It is therefore imperative for osteopaths to:
Prioritize less invasive techniques , such as gentle mobilizations, particularly in at-risk groups (young women, patients with a history of trauma).
Perform rigorous screenings to identify red flags (dizziness, history of vascular pathologies, unusual headaches).
Inform patients of potential risks and available alternatives.
Reported incidence rates of VBS associated with cervical manipulation vary considerably due to differences in study methodologies and diagnostic criteria. The following is a breakdown of the estimates:
- Maigne (1972): Suggests an extremely low incidence, indicating that such events are very rare compared to the number of manipulations carried out.
- Cyriax (1978): Estimated a rate of 1 in 10 million manipulations, which implies that VBS is an extremely rare complication.
- Hosek et al. (1981): reported a similarly low rate of 1 per million, reinforcing the rarity of this adverse event.
- Gutmann (1983) and Dvorak and Orelli (1985): found slightly higher rates (2 to 3 per million), which still reflect a low overall risk.
- Rivet and Milburn: provided a wider range, from 1 in 50,000 to 1 in 5 million manipulations. This variability may reflect differences in study populations and definitions of adverse events.
- Boyle et al. reported a higher rate of 6 manipulations per 100,000. This figure is significantly higher than others and could be due to different reporting criteria or practices.
- Patijn: The rate is estimated at 1 in 518,886 manipulations, which is at the lower end of the spectrum found in other studies.
Factors influencing risk
- Pre-existing conditions: Patients with certain risk factors, such as pre-existing vascular conditions or anatomical variations, may be at higher risk of adverse events.
- Technique and experience: The skill and experience of the practitioner, as well as the specific techniques used, can influence the risk of VBS.
- Diagnostic practices: The accuracy of diagnosis and reporting of adverse events may vary, affecting reported incidence rates.
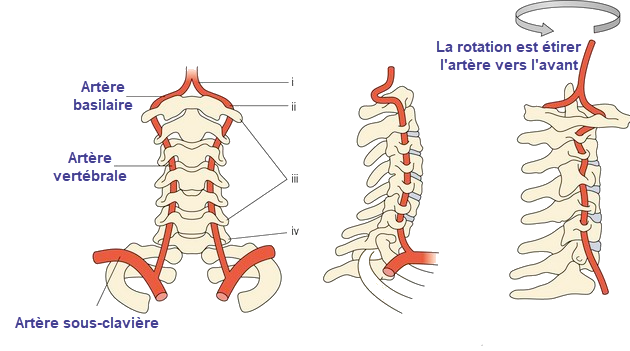
The left side of the image shows the connection between the subclavian artery (from which the vertebral artery arises) and the basilar artery. This anatomical configuration highlights the vulnerability of these arteries to mechanical stress.
The right side of the image illustrates the effect of rotational movements of the neck on the vertebral artery. When the neck is rotated, the artery is stretched forward, which can increase the mechanical stress on its wall. These stresses can sometimes reduce blood flow, particularly in patients with pre-existing pathologies or malformations.
This understanding is crucial for healthcare professionals, such as osteopaths, as it highlights the importance of carefully assessing cervical movement to avoid vascular complications. It also highlights the importance of considering vascularity in therapeutic approaches.
Pathophysiology of Vertebral Artery Dissection
Vertebral artery dissection (VAD) is a common cause of stroke in young adults. It results from injury to the arterial wall, causing separation of the artery layers and the formation of an intramural hematoma. This complex condition involves various pathophysiological mechanisms, including mechanical, structural, and hemodynamic factors. This text explores the main stages and mechanisms underlying VAD.
Structure and Functions of the Vertebral Artery
The vertebral artery is an important artery of the cerebrovascular system. It arises from the subclavian artery, crosses the transverse foramina of the cervical vertebrae, and then enters the skull through the foramen magnum. Its wall is composed of three layers: the intima, the media, and the adventitia.
- Intima : Inner layer, composed of an endothelium resting on a basal lamina.
- Media : Muscular and elastic layer, responsible for mechanical resistance and modulation of vascular diameter.
- Adventitia : Outer layer, rich in collagen fibers and vasa vasorum.
Dissection usually affects the intima and/or media, leading to local weakening and secondary complications.
Triggering Mechanisms of Dissection
- Mechanical Trauma Trauma, whether major (road accidents) or minor (sudden neck movements, spinal manipulations), is a common trigger. These forces can cause an initial injury to the intima, exposing the underlying layer and promoting blood entry into the arterial wall.
- Genetic and Connective Factors Certain genetic abnormalities predispose to AVD, including connective tissue disorders such as Ehlers-Danlos syndrome or Marfan syndrome. These diseases alter the structure of collagen and elastin, weakening the arterial wall and increasing susceptibility to dissection.
- Hemodynamic Factors Curved regions of the vertebral artery, particularly in the intraforaminal and intracranial segments, are exposed to high shear forces. These chronic mechanical stresses can cause micro-tears of the intima.
- Inflammation and Vascular Alterations Inflammatory conditions, such as giant cell arteritis or systemic infections, can weaken vessels. Infections, in particular, can cause endothelial micro-lesions, promoting the development of dissection.
Formation of Intramural Hematoma
Intimal rupture allows blood under pressure to enter the media, creating an intramural hematoma. This hematoma can spread longitudinally, increasing the risk of complications. The effects of this hematoma depend on its location:
- Luminal Compression : The hematoma can compress the arterial lumen, resulting in stenosis or complete occlusion. This reduction in blood flow can cause cerebral ischemia.
- Creation of a False Aneurysm : If the hematoma spreads outward by rupturing the adventitia, a false aneurysm may form, increasing the risk of arterial rupture.
Ischemia and Embolization
One of the main complications of AVD is cerebral ischemia, often due to arterial embolism. Two main mechanisms are involved:
- Localized Thrombosis Turbulence of blood flow at the site of dissection promotes platelet aggregation and thrombus formation. These thrombi can embolize to distal branches, causing cerebral infarction.
- Reduced Blood Flow Severe stenosis or occlusion results in decreased blood flow to areas dependent on the vertebral artery, including the brainstem, cerebellum, and occipital lobes.
Risk Factors and Predispositions
Several factors can increase the likelihood of a DAV:
- Smoking : Contributes to inflammation and endothelial dysfunction.
- Hypertension : Increases mechanical stress on arterial walls.
- Hypercholesterolemia : Promotes atheromatous plaques, predisposing to mechanical lesions.
Repair and Long-Term Consequences
The healing process of AVD involves a gradual rebuilding of the arterial layers. However, complications may persist:
- Restenosis : Wall remodeling can lead to fibrosis and chronic reduction in arterial caliber.
- Persistent Aneurysms : Some dissections do not close completely, leaving areas of residual dilation.
Vertebral artery dissection
The vertebral artery, a vital blood vessel supplying blood to the posterior regions of the brain, is particularly vulnerable to injury during certain manipulations. This vulnerability is especially acute as the artery passes from the transverse foramen of the second cervical vertebra (C2, also called the axis) to that of the first cervical vertebra (C1, the atlas). As the vertebral artery exits the transverse foramen of C2, it must undergo an abrupt change of direction to enter the transverse foramen of C1. This abrupt change of direction exposes the artery to considerable risk, particularly during cervical manipulations.
Cervical manipulation, which often involves rotational movements of the head and neck, places significant pressure on the vertebral artery, particularly at the C2 level. During these procedures, the vertebral artery can be stretched, compressed, or twisted, potentially leading to dissection, a serious condition in which the inner wall of the artery tears. When the vertebral artery is already compromised or insufficient, its vulnerability to injury increases significantly. The risk of such injury can be increased by the mechanical forces applied during cervical manipulation.
Vertebral artery dissection is a major concern in the context of cervical manipulation. Research has shown that cervical manipulation can independently increase the risk of vertebral artery dissection (VAD) and subsequent stroke. Smith et al. suggested that the risk of VAD with stroke after cervical manipulation may increase approximately sixfold. This increased risk underscores the need for careful assessment and consideration before performing manipulative procedures on patients with potential vertebrobasilar insufficiency.
The clinical presentation of vertebral artery dissection often includes symptoms such as dizziness, vertigo, and other signs of decreased cerebral blood flow. These symptoms can be distressing and may require urgent medical evaluation. Although vertebral artery dissection can occur in younger individuals, it is more commonly seen in older populations, reflecting a higher overall risk with age.
Statistical data on the incidence of ventricular dysfunction after cervical manipulation indicate a variable risk range. Reports suggest that the occurrence of ventricular dysfunction after cervical manipulation ranges from 1 in 10,000 to 1 in 2 million procedures (references 3-4). Despite these low incidence rates, the potential severity of ventricular dysfunction requires a cautious approach.
As a therapist or healthcare provider, it is essential to recognize the risk of vertebral artery dissection. Although the likelihood of such an adverse event is minimal, it is still essential to assess the integrity of the vertebral artery before undertaking any cervical manipulation. This pre-manipulatory assessment helps ensure patient safety and mitigate the risk of potentially serious complications.
In summary, the anatomical course of the vertebral artery and its sensitivity to mechanical stress highlight the importance of careful consideration and assessment during cervical manipulation. Understanding the risks associated with vertebral artery dissection and implementing appropriate safety measures can significantly reduce the likelihood of adverse events and improve patient safety in clinical practice.
Vertebral artery trauma following cervical manipulation occurs primarily in its atlanto-axial component, which is stretched forward during rotation.
Vertebral artery dissection (VAD) is a rare but serious condition that can lead to major neurological complications, including stroke. VAD occurs when a tear in the vertebral artery wall allows blood to leak between the layers of the arterial wall, creating a hematoma that can partially or completely obstruct blood flow to the brain. Recognizing the symptoms of this condition is essential to enable timely intervention and limit complications.
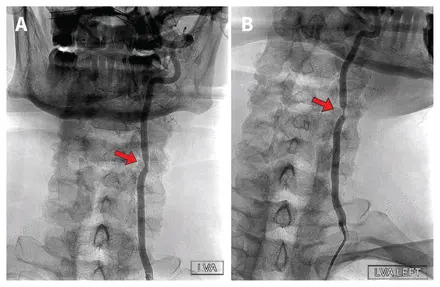
(A) When the patient is at rest with the head in a neutral position and looking forward, there is a slight narrowing of the left vertebral artery (LVA) in the mid-cervical region, caused by hypertrophy of the uncovertebral joint between the third and fourth vertebrae (arrow).
(B) When the patient turns his head to the left, there is a significant compromise of the LVA lumen, attributable to compression of the blood vessel by the bony structure (arrow).
Note: LVG = AVG, LVG Left = AVG gauche .
“Dynamic cerebral angiographic examination of a 59-year-old man with vertebrobasilar insufficiency” by Anna Luisa Kühn, from CMAJ (vol. 195, no. 14, E533) , distributed under CC BY-NC-ND 4.0 / no modifications made.
Symptoms of vertebrobasilar insufficiency
The symptoms of vertebrobasilar insufficiency (VBI) are diverse and can significantly impact a person’s quality of life. They result from reduced blood flow to the posterior regions of the brain, including the brainstem, cerebellum, and occipital lobes. One of the most common symptoms associated with VBI is dizziness, which can manifest as a feeling of lightheadedness or spinning (vertigo). This dizziness can be severe and disabling, leading to loss of balance and an increased risk of falling. Patients may also experience a feeling of unsteadiness, which can interfere with their ability to walk or perform daily activities.
Visual disturbances are another important symptom of VBI. People may report blurred vision, double vision (diplopia), or transient vision loss. These visual symptoms occur because the brainstem, which is essential for processing visual information, is affected by reduced blood supply. Additionally, patients may experience difficulty with depth perception and coordination, making tasks that require precise movements, such as writing or buttoning a shirt, difficult.
Hearing-related symptoms may also be present in visual hearing impairment. Tinnitus, or ringing in the ears, is a common complaint, and some people may experience hearing loss or changes in auditory perception. This can be particularly distressing and can exacerbate difficulties experienced in daily life.
Neurological symptoms associated with VBI include speech and cognitive function problems. Patients may experience slurred speech, difficulty finding the right words, or problems understanding spoken language. Cognitive impairments may include confusion, memory problems, or difficulty concentrating. These symptoms occur because the brainstem, which plays a crucial role in many of these functions, is compromised.
In addition to these symptoms, people with VBI may experience sudden weakness or numbness, usually affecting one side of the body. This may be a sign of a transient ischemic attack (TIA) or mini-stroke, which are related to reduced blood flow in the vertebrobasilar system. In severe cases, VBI can lead to full-blown strokes, characterized by more profound weakness, paralysis, or loss of sensation on one side of the body, as well as difficulty speaking or understanding.
Coordination problems are also common, with patients often having difficulty with fine motor skills or maintaining balance. This can result in a wobbly gait or difficulty performing tasks that require hand-eye coordination. Feeling unsteady and lacking control over one’s movements can significantly affect a person’s ability to perform daily activities and maintain independence.
Other systemic symptoms may include nausea, vomiting, and a general feeling of malaise. These symptoms are often associated with the dizziness and vertigo that occur in IVB. In some cases, patients may also experience a feeling of pressure in the head or a headache, although these symptoms are less specific to IVB and may overlap with other conditions.
Overall, the symptoms of vertebrobasilar insufficiency are multiple and can vary in intensity. The combination of dizziness, visual and hearing disturbances, neurological deficits, and coordination problems can significantly affect an individual’s functional ability and quality of life. Early recognition and management of these symptoms are essential to prevent progression and reduce the risk of more serious outcomes, such as stroke. Accurate diagnosis and targeted treatment strategies are essential to effectively manage vertebrobasilar insufficiency and improve patient outcomes.
Risk factors for vertebral artery dissection
Vertebral artery dissection (VAD) is a rare but serious, often underdiagnosed vascular condition that can lead to major neurological complications such as stroke. Although its incidence is relatively low, it frequently affects young, healthy adults. Multiple risk factors, both intrinsic and extrinsic, contribute to the development of this condition, highlighting a complex interplay between genetic predispositions, mechanical influences, lifestyle, and medical conditions.
Genetic factors play an important role in susceptibility to AVD. Certain inherited disorders, particularly those affecting connective tissue, increase the risk of arterial tears. Ehlers-Danlos syndrome type IV is a well-known example of a genetic disorder associated with weak vascular walls. This rare condition causes a collagen defect that makes arteries more fragile and prone to tearing under normal mechanical stress. Similarly, Marfan syndrome, another inherited connective tissue disorder, causes decreased vascular elasticity and can predispose to dissections. Other congenital structural abnormalities, such as vertebral artery hypoplasia, where the artery is underdeveloped, also increase the risk of vascular damage.
Mechanical factors are another major risk category, as the vertebral arteries are exposed to significant stress due to their location in the neck. Direct trauma, such as that occurring during a car accident or a fall, is a common cause of dissection. However, repetitive strain injuries can also play a role, particularly in athletes participating in contact or impact sports, such as football or martial arts. These accumulated strain injuries can gradually weaken the arterial walls, increasing their vulnerability. Furthermore, certain extreme neck movements, such as hyperextension or rapid rotation, can place excessive stress on the vertebral artery, promoting a tear. Neck manipulation performed as part of therapeutic practices, such as osteopathy or chiropractic, has also been linked to cases of arterial dissection, although this link remains debated in the medical community.
Lifestyle also contributes to the occurrence of VAD, primarily through its effects on overall vascular health. Smoking is a well-established risk factor, as it promotes atherosclerosis and directly damages vessel walls, making them more fragile and susceptible to tearing. Similarly, high blood pressure places constant stress on arteries, increasing their vulnerability to dissection. Excessive or poorly managed physical activity can also cause a sudden increase in blood pressure, leading to stress on vessel walls and an increased risk of VAD. In contrast, regular, moderate physical activity is beneficial for vascular health and can help reduce the risk.
Infections and inflammations are another potential cause of vertebral artery weakness. Certain upper respiratory infections, such as those caused by viruses or bacteria, can be associated with arterial dissection. These infections cause vascular inflammation, increasing the susceptibility of arterial walls to injury. Furthermore, chronic inflammatory diseases such as systemic lupus erythematosus or rheumatoid arthritis can weaken vessels due to persistent inflammatory processes. These inflammations damage the inner layers of the arteries, making them more vulnerable to mechanical forces and hemodynamic stress.
Hormonal factors and gender-specific conditions also influence AVD. In women, pregnancy is a recognized risk factor due to the hormonal and hemodynamic changes it induces. These changes make arterial walls more fragile and susceptible to tearing, particularly during the third trimester or immediately after childbirth. Hormonal fluctuations may also influence vascular health in general, although their precise role in arterial dissection requires further research.
Local vascular abnormalities also increase the risk of VAD. Excessive tortuosity or congenital malformations of the vertebral arteries can lead to increased stress on the arterial walls during neck movements. Similarly, conditions such as atherosclerosis, although more common in older adults, can weaken vessels and make younger adults more vulnerable to dissection. These vascular abnormalities also increase the risk of clot formation, which can worsen complications associated with VAD.
Finally, psychological stress plays an indirect but significant role in the development of AVD. Severe stress can cause elevated blood pressure, which puts additional pressure on arterial walls. Additionally, risky behaviors often associated with stress, such as smoking or unsupervised intense physical activity, can also increase the risk of dissection. Chronic stress can also have adverse effects on overall vascular health, exacerbating other predisposing factors.
Thus, vertebral artery dissection results from a complex combination of genetic predispositions, mechanical and environmental factors, as well as lifestyle behaviors. Special attention must be paid to these elements to identify individuals at risk and prevent serious complications of this pathology.
Examples of documented clinical cases: Complications related to cervical manipulations
Cervical manipulation, while useful in many therapeutic settings, is not without risk. The medical literature reports cases where complications have occurred, highlighting the importance of caution in its application. These cases offer valuable lessons for osteopathic practitioners, encouraging them to carefully assess patients and follow strict safety protocols. Here is a presentation of published clinical cases that illustrate the risks associated with these practices.
Section Development: Case Studies on Complications Related to Cervical Manipulation
1. Dissection of the vertebral artery after cervical manipulation
Source : IMR Press
A 30-year-old man, in good general health and with no significant medical history, presented with persistent moderate neck pain, aggravated by his desk job. He underwent cervical manipulation with forced rotation at the C1-C2 vertebrae. Shortly after the session, he experienced severe pain in the back of his neck, followed by dizziness, blurred vision, and loss of coordination.
Lesson learned : This case highlights that even in young adults with no apparent risk factors, cervical manipulations involving rotations should be performed with caution. A prior functional assessment of vertebral artery integrity could have prevented this event.
Diagnosis : MRI and angiography reveal a dissection of the left vertebral artery, resulting in ischemia in the cerebellar territory, also known as Wallenberg syndrome. This condition is characterized by involvement of the posterior brainstem.
Clinical course : The patient was urgently hospitalized and treated with anticoagulants to prevent further complications. After several months of neurological rehabilitation, he partially recovered, but still has mild after-effects such as instability when walking.
2. Syndrome de Wallenberg post-manipulation cervicale
Source : IMR Press
A 25-year-old woman presents with chronic migraines associated with cervical stiffness, which she attributes to prolonged hours spent in front of a computer. During the session, a cervical manipulation involving high-velocity extension and rotation is performed. Shortly after the manipulation, she reports dizziness, nausea, and slurred speech.
Lesson learned : This case highlights the importance of rigorous screening for vascular risk factors, even in young adults. Any migraine associated with neck stiffness should alert you to a potential risk of vascular pathology.
Diagnosis : Neurological examination reveals ataxia (loss of coordination), and an MRI shows an infarct located in the territory of the right vertebral artery, confirming Wallenberg syndrome. This syndrome results from an arterial occlusion affecting the brainstem.
Clinical course : The patient was treated with antiplatelet drugs and neurological rehabilitation. Despite functional recovery after six months, subtle coordination disorders persist.
3. Dissection of the vertebral artery in a full-term pregnant woman after cervical manipulation
Source : REVMED
A 39-year-old pregnant woman at 38 weeks’ gestation presents with neck pain associated with pregnancy-related muscle tension. Gentle cervical manipulation is performed to relieve the pain, but a few hours after the session, she begins to experience severe dizziness, nausea, and vomiting.
Lesson learned : This case highlights the increased vulnerability of pregnant patients to certain complications. Cervical manipulation should be avoided in pregnant women, particularly in late pregnancy, due to hemodynamic and hormonal changes.
Diagnosis : An MRI and CT angiogram show a dissection of the left vertebral artery, likely triggered by cervical manipulation. This type of complication is rare but particularly concerning in late pregnancy.
Clinical course : The patient was hospitalized and treated with anticoagulants appropriate to her condition. Her delivery was uneventful, but close postpartum monitoring was necessary to avoid recurrences.
4. Dissection of the vertebral artery after cervical manipulation
Source : Cardiological Realities
A 40-year-old man suffering from chronic neck pain after a minor accident (whiplash) consulted for osteopathic treatment. After cervical manipulation involving traction and rotation, he developed acute neck pain followed by neurological symptoms: muscle weakness and visual disturbances.
Lesson learned : This case highlights the importance of assessing a history of cervical trauma before considering manipulation. An alternative approach, such as gentle mobilizations, could have reduced the risk.
Diagnosis : A left vertebral artery dissection is diagnosed, resulting in an ischemic stroke.
Clinical course : The patient was admitted to intensive care, where he received anticoagulant treatment and neurological support. Prolonged rehabilitation was required to recover some of his functional abilities.
5. Wallenberg syndrome secondary to vertebral artery dissection after cervical manipulation
Source : IMR Press
A 45-year-old man presented with neck pain with no specific medical history. After a single neck manipulation, involving high-velocity lateral rotation, he rapidly developed dizziness, dysphagia (difficulty swallowing), and unilateral weakness.
Lesson learned : This case highlights the importance of a personalized approach. Preliminary vascular function tests, such as the passive cervical rotation test, can help identify at-risk patients before any manipulation.
Diagnosis : A brain MRI revealed a dissection of the left vertebral artery resulting in Wallenberg syndrome. This syndrome, caused by ischemia of the posterior brainstem, causes significant motor and sensory disturbances.
Clinical evolution : Despite rapid intervention with anticoagulants, the patient presents long-term neurological sequelae, notably postural instability.
Alternatives to cervical manipulation in osteopathic treatments
Cervical manipulation, while effective in many cases, carries a potential risk, particularly in patients with vulnerability factors such as vertebrobasilar insufficiency, joint instability, or a history of vascular disease. For these populations, it is essential to prioritize less invasive osteopathic techniques that ensure therapeutic efficacy while minimizing risks. Here’s an exploration of alternative approaches, their benefits, and their clinical indications.
1. Gentle cervical mobilizations
Gentle mobilizations are a safe and effective alternative to manipulation. These techniques aim to restore joint mobility without sudden movements or forced rotations. They are characterized by moderate amplitudes and controlled speeds.
- Description of the technique :
- Mobilizations involve passive movements of the cervical segments performed by the practitioner.
- These movements include lateral tilts, light rotations and flexion-extensions, adapted to the patient’s ability.
- Benefits :
- No excessive stress on vascular or joint structures.
- Allows muscle relaxation and progressive joint release.
- Reduces pain without causing discomfort or risk of complications.
- Indications :
- Elderly patients with osteoporosis or cervical osteoarthritis.
- Patients with vascular or neurological red flags.
- Subjects who are anxious or apprehensive about manipulation.
2. Techniques myofasciales
Myofascial release techniques focus on the soft tissues surrounding muscles and fascia. These structures play a key role in cervical dynamics and are often implicated in movement restrictions or pain.
- Description of the technique :
- Gentle manual work on the fascia and cervical muscles to release tension.
- Combination of light pressure and progressive stretching to promote tissue relaxation.
- Benefits :
- Reduces muscle tension that limits cervical mobility.
- Improves local vascularization and reduces inflammation.
- Suitable for patients with acute or chronic pain.
- Indications :
- Cervical tension syndromes associated with prolonged postures (e.g., office work).
- Cervical mobility restrictions of muscular or fascial origin.
- Patients with increased sensitivity to touch or manipulation.
3. Cranial techniques
Cranial techniques, commonly used in osteopathy, involve very gentle manipulations of the bones of the skull and upper cervical region. These approaches are based on the idea of physiological micro-movement between bony structures and soft tissues.
- Description of the technique :
- Extremely light pressure applied to the cranial and upper cervical regions (C0-C1-C2).
- Objective: improve fluid circulation and restore overall mechanical balance.
- Benefits :
- Non-invasive and suitable for all ages, including infants and the elderly.
- Promote relaxation and reduce chronic pain without the risk of vascular complications.
- Indications :
- Tension headaches or migraines.
- Joint dysfunction at the craniocervical junction.
- Functional disorders associated with stress.
4. Functional techniques
Functional techniques rely on the principle of induction, following the body’s natural movements and mechanical preferences to relieve tension and restore mobility.
- Description of the technique :
- The practitioner supports the natural micro-movements of the cervical structures until relaxation is achieved.
- The techniques are performed gently, without exceeding the patient’s comfort limits.
- Benefits :
- Very safe, they respect the patient’s physiological capacities.
- Effective for acute or post-traumatic pain.
- Rapid pain reduction with minimal intervention.
- Indications :
- Patients with reduced mobility due to recent trauma (e.g., whiplash).
- Acute conditions requiring a gentle approach to avoid worsening.
5. Visceral techniques
Although the cervical region is primarily musculoskeletal, visceral tension can contribute to cervical dysfunction, particularly via the fascia that connects internal structures.
- Description of the technique :
- Work on the visceral fascia (e.g., esophagus, upper thorax) to release tension that can affect the cervical spine.
- Benefits :
- Holistic approach that considers the links between internal organs and neck pain.
- Reduces chronic tensions that are sometimes resistant to purely structural approaches.
- Indications :
- Patients with neck pain associated with digestive or respiratory disorders.
- Chronic cervical restrictions of postural origin.
6. Active rehabilitation exercises
Active exercises, although performed by the patient, are guided and monitored by the osteopath to restore cervical function gradually.
- Description :
- Gentle stretching, range of motion exercises and targeted muscle strengthening.
- Includes proprioceptive exercises to improve motor control.
- Benefits :
- Prevents dependence on passive care.
- Promotes patient autonomy and prevents recurrences.
- Improves posture and cervical stability.
- Indications :
- Monitoring of patients after an acute or post-traumatic period.
- Patients with recurrent neck pain due to muscle weakness.
7. Importance of a personalized approach
It is crucial that the osteopath carefully assesses each patient to determine the most appropriate approach for their needs. Alternatives to cervical manipulation not only minimize risks but also provide effective and individualized treatment.
These techniques, combined with rigorous assessment and personalized monitoring, ensure comprehensive care that respects both the safety and expectations of the patient.
Vertebrobasilar insufficiency tests
Vertebrobasilar insufficiency (VBI) tests are used for preventive purposes before performing cervical manipulations or mobilizations.
These tests are provocative in nature and are performed to test the collateral and vertebrobasilar blood supply to the brain. They are performed to test the collateral and vertebrobasilar blood supply to the brain to detect signs and symptoms of vertebral artery pathology, which may pose a risk prior to manipulation.
1. Passive test to verify the integrity of the vertebral artery
- Place the patient in the supine position and perform passive extension and lateral flexion of the head and neck.
- Passively rotate your neck to the same side and hold this position for about 30 seconds.
- Repeat the test with a head movement to the opposite side.
- The test is considered positive if there is arm drop, loss of balance, or hand pronation; a positive result indicates decreased blood supply to the brain.
- Other positive symptoms:
- Dizziness
- Tinnitus
- Dizziness
- Nystagmus
- Paresthesia
- Dysarthrie
- Diplopia
- Dysphagia
2.Active vertebral artery test(Deklein)
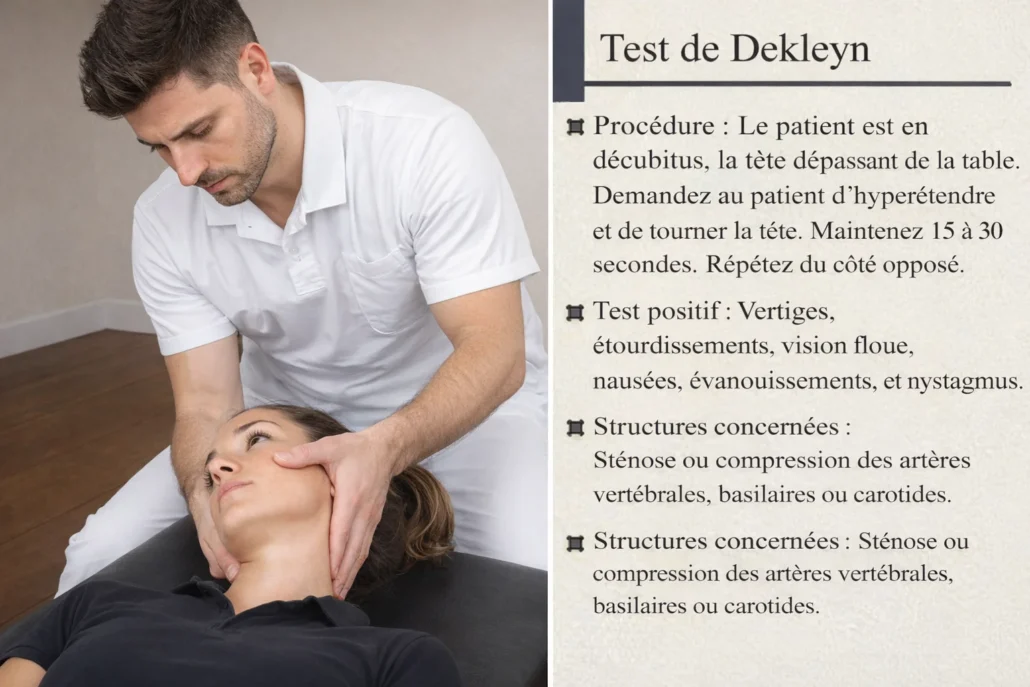
- Patient in supine position, head off the table.
- Ask the patient to hyperextend and rotate the head.
- Hold this position for 15 to 30 seconds.
- Repeat the reverse operation.
Positive test: Dizziness, lightheadedness, blurred vision, nausea, fainting, and nystagmus. –
Affected structures: Stenosis or compression of the vertebral, basilar or carotid artery.
If the presence of a BVI is evident in a patient, the practitioner should immediately discontinue the provocation test and return the patient’s neck to a neutral position (Rivett et al., 2005). Manipulative procedures should be discontinued and the patient referred to a specialist for further medical evaluation.
Safety protocols for osteopaths: Practical recommendations
Cervical manipulation, while effective in many cases, requires a cautious approach due to potential risks related to vertebrobasilar circulation. To ensure patient safety, osteopaths must adhere to strict protocols to identify risk factors, recognize red flags, and act accordingly. Here are some practical recommendations to follow.
1. In-depth initial assessment
The first step in ensuring the safety of cervical manipulation is a complete clinical assessment, including:
- Detailed medical history :
- Identify a history of vascular disease, stroke, hypertension, or high cholesterol.
- Check for risk factors such as smoking, advanced age or a family history of cardiovascular disease.
- Explore symptoms suggesting vertebrobasilar insufficiency (VBI): dizziness, visual disturbances, nausea, imbalances.
- Careful clinical examination :
- Perform specific tests to assess vascular integrity, such as the cervical rotation test (does it cause dizziness or visual disturbances?).
- Palpate the cervical region for any abnormal stiffness or pain that could indicate a structural problem.
- Use of standardized questionnaires :
- Screening questionnaires, such as those used for cardiovascular risk, can help identify warning signs.
2. Identifying red flags
Certain signs or symptoms should alert the osteopath to a potential contraindication to cervical manipulation:
- Neurological symptoms :
- Transient vision loss.
- Muscle weakness or numbness.
- Coordination problems or dysarthria (difficulty speaking).
- Vascular signs :
- Dizziness or vertigo exacerbated by specific neck movements.
- Severe and unusual neck pain.
- History of arterial dissection or suspicion of dissection.
- Other red flags :
- Sudden and intense migraine.
- History of recent cervical trauma (e.g., whiplash).
- Presence of inflammatory or infectious diseases that can affect the arteries.
Faced with these red flags, it is imperative to suspend all cervical manipulation and refer the patient to a specialist for further examinations (neurologist, angiologist).
3. Specific functional tests
Before performing cervical manipulation, functional tests are used to check vascular tolerance:
- Passive cervical rotation test :
- The practitioner gently turns the patient’s head to one side, while observing for the appearance of symptoms such as dizziness or nausea.
- Take the test on both sides and compare the answers.
- Spinal compression test (performed with caution):
- Allows assessment of vertebral artery reactivity under certain constraints.
In case of doubt or positive results from these tests, it is preferable not to proceed with any manipulation and to seek a therapeutic alternative.
4. Use of alternatives to cervical manipulation
If doubts remain regarding the patient’s vascular integrity, the osteopath may favor less invasive techniques, such as:
- Soft mobilizations :
- Techniques aimed at restoring joint mobility without sudden movements or forced rotations.
- Techniques myofasciales :
- Work on muscular and fascial tensions to release cervical structures without stress on the arteries.
- Cranial or indirect approaches :
- Non-invasive techniques that reduce mechanical stress on the cervical region.
These approaches guarantee safe care while respecting the patient’s therapeutic needs.
5. Continuing education and evidence-based practice
Osteopaths must keep their skills up to date through:
- Training on vascular pathologies :
- Participate in workshops or seminars on the management of patients at risk of IVB.
- Follow scientific advances concerning cervical manipulation and vascular risks.
- Evidence-based approach :
- Adopt evidence-based techniques, drawing on recent studies to adapt clinical practices.
6. Protocol in case of complications
If a complication occurs during or after cervical manipulation, the practitioner must follow a clear protocol:
Ensure regular follow-up with the patient to assess progress.
Quickly recognize emergency signs :
Symptoms of arterial dissection: severe neck pain, sudden visual or neurological disturbances.
Stroke symptoms: sudden paralysis, difficulty speaking, facial asymmetry.
Intervene immediately :
Stop treatment and place the patient in a resting position.
Call emergency services for immediate medical attention.
Documentation and monitoring :
Record events precisely to inform medical teams.
If the presence of BVI is evident in a patient, the practitioner should immediately discontinue provocation testing and return the patient’s neck to a neutral position (Rivett et al., 2005). Manipulation procedures should be discontinued and the patient referred to a specialist for further medical examination.
Quizz
Quizz 1
What is Vertebrobasilar Insufficiency (VBI)?
a) A condition affecting the carotid arteries
b) A reduction in blood flow to the anterior brain regions
c) A reduction in blood flow to the posterior brain regions
d) An increase in blood flow to the spinal cord
e) A condition related to upper limb circulation
2. How do the vertebral arteries enter the cervical spine?
a) Through the foramen magnum
b) Through the transverse foramen of each cervical vertebra from C1
c) Through the transverse foramen of each cervical vertebra from C6
d) Directly from the subclavian artery to the brainstem
e) Through the sacral foramina
3. What is a significant mechanical stress placed on the vertebral arteries during cervical movements?
a) Compression and stretching
b) Increased blood flow
c) Reduced arterial tension
d) Enhanced artery elasticity
e) None of the above
4. What does cervical manipulation often involve?
a) Applying specific forces to the lumbar spine
b) Applying specific forces to the cervical spine
c) Applying general pressure to the entire spine
d) Massaging the sacral area
e) Performing passive leg movements
5. Which of the following is NOT a reported incidence rate of vertebrobasilar stroke (VBS) related to cervical manipulation?
a) 1 in 10 million manipulations
b) 1 in 100,000 manipulations
c) 1 in 1 million manipulations
d) 1 in 5 million manipulations
e) 6 in 100,000 manipulations
6. Which test involves placing the patient supine and performing passive extension and lateral flexion of the head?
a) Dekleyn’s Test
b) Schober’s Test
c) Passive Test for Vertebral Artery Integrity
d) Active Test for Vertebral Artery Integrity
e) Tinel’s Sign
7. What symptoms are commonly associated with vertebrobasilar insufficiency (VBI)?
a) Tingling in the toes
b) Headaches, dizziness, and visual disturbances
c) Sudden muscle spasms in the back
d) Lower back pain and stiffness
e) Cold extremities and reduced grip strength
8. What is a critical concern related to cervical manipulation and vertebral artery dissection?
a) Decreased blood flow in the carotid arteries
b) Increased risk of vertebral artery dissection
c) Improved circulation to the spinal cord
d) Enhanced flexibility of the lumbar spine
e) None of the above
9. How does the mechanical stress applied during cervical rotation affect the vertebral arteries?
a) It improves blood flow through the arteries
b) It causes temporary or persistent reductions in blood flow
c) It has no significant impact on blood flow
d) It increases arterial elasticity
e) It enhances vertebral artery strength
10. What should be done if vertebrobasilar insufficiency is evident during testing?
a) Continue with cervical manipulation
b) Apply more pressure during the test
c) Discontinue manipulation and refer the patient to a specialist
d) Perform additional manual therapy
e) Ignore the symptoms as they are non-critical
Answers
- c) A reduction in blood flow to the posterior brain regions
- c) Through the transverse foramen of each cervical vertebra from C6
- a) Compression and stretching
- b) Applying specific forces to the cervical spine
- b) 1 in 100,000 manipulations
- c) Passive Test for Vertebral Artery Integrity
- b) Headaches, dizziness, and visual disturbances
- b) Increased risk of vertebral artery dissection
- b) It causes temporary or persistent reductions in blood flow
- c) Discontinue manipulation and refer the patient to a specialist
Quizz 2
Which anatomical feature is particularly notable about the vertebral arteries in the cervical region?
a) They enter the vertebrae directly from the heart
b) They ascend through the transverse foramina of the cervical vertebrae
c) They are found only in the lumbar spine
d) They pass through the sacral foramina
e) They originate from the internal carotid artery
2. What is the primary risk factor for vertebral artery dissection during cervical manipulation?
a) Reduced vertebral artery elasticity
b) Sharp directional change of the artery
c) Increased blood flow through the artery
d) High levels of physical fitness
e) Decreased mechanical stress
3. What type of symptoms might indicate vertebral artery dissection?
a) Lower back pain and stiffness
b) Unilateral neck pain and sudden headache
c) Pain in the extremities
d) Cold hands and feet
e) Abdominal cramping
4. What is the purpose of the passive test for vertebral artery integrity?
a) To assess overall spinal flexibility
b) To evaluate the integrity of the vertebral artery during passive head movements
c) To measure leg strength
d) To test respiratory function
e) To determine overall cardiovascular health
5. How is the risk of vertebrobasilar stroke (VBS) reported to vary according to the studies?
a) Consistently high across all studies
b) Ranges from extremely rare to relatively frequent
c) Identical in all studies
d) Only reported as common in older studies
e) Not reported in recent studies
6. What does the Dekleyn’s Test involve?
a) Assessing the integrity of the lumbar spine
b) Hyperextending and rotating the head while supine
c) Applying pressure to the thoracic spine
d) Measuring spinal range of motion
e) Performing passive leg extensions
7. Which of the following is NOT a symptom of vertebrobasilar insufficiency (VBI)?
a) Tinnitus
b) Blurred vision
c) Dizziness
d) Chest pain
e) Slurred speech
8. According to the text, which of the following conditions is a risk factor for vertebral artery dissection?
a) Recent upper respiratory infection
b) Regular physical exercise
c) Low blood pressure
d) Balanced diet
e) Frequent hydration
9. What should be done if a positive result is obtained from vertebrobasilar insufficiency testing?
a) Continue with the planned cervical manipulation
b) Adjust the manipulation technique
c) Discontinue the manipulation and refer the patient for further evaluation
d) Perform additional manipulative procedures
e) Ignore the result as it is not significant
10. How is cervical manipulation related to the risk of vertebral artery dissection?
a) It is unrelated to the risk
b) It decreases the risk significantly
c) It can independently increase the risk of vertebral artery dissection
d) It has no impact on vertebral artery dissection
e) It improves arterial integrity
Answers
- b) They ascend through the transverse foramina of the cervical vertebrae
- b) Sharp directional change of the artery
- b) Unilateral neck pain and sudden headache
- b) To evaluate the integrity of the vertebral artery during passive head movements
- b) Ranges from extremely rare to relatively frequent
- b) Hyperextending and rotating the head while supine
- d) Chest pain
- a) Recent upper respiratory infection
- c) Discontinue the manipulation and refer the patient for further evaluation
- c) It can independently increase the risk of vertebral artery dissection
Quizz 3
1. What is the primary consequence of vertebrobasilar insufficiency (VBI)?
a) Increased blood flow to the brainstem
b) Impaired blood flow to the posterior regions of the brain
c) Enhanced coordination and balance
d) Decreased sensitivity to pain
e) Improved cognitive function
2. In which part of the cervical spine does the vertebral artery undergo a significant directional change?
a) C3-C4
b) C5-C6
c) C1-C2
d) C7-T1
e) C2-C3
3. What does the incidence rate of vertebrobasilar stroke (VBS) related to cervical manipulation typically reflect?
a) A high frequency of complications
b) A consistent risk across different studies
c) A low overall risk with considerable variability
d) No reported cases in recent studies
e) A risk that increases with each manipulation
4. What are common symptoms of vertebrobasilar insufficiency (VBI) that affect visual perception?
a) Double vision and blurred vision
b) Deafness and tinnitus
c) Sensory loss in the extremities
d) Seizures and tremors
e) Chronic cough and sore throat
5. Which of the following is NOT a common symptom of vertebral artery dissection?
a) Headaches
b) Neck pain
c) Visual disturbances
d) Difficulty swallowing
e) Joint pain in the knees
6. What is the primary goal of performing vertebrobasilar insufficiency tests before cervical manipulation?
a) To determine the overall spinal health
b) To assess the integrity of vertebral and basilar blood supply
c) To measure the patient’s pain tolerance
d) To evaluate muscle strength in the neck
e) To check for signs of infection
7. How does cervical manipulation potentially affect the vertebral arteries?
a) It increases blood flow through the arteries
b) It can place mechanical stress on the arteries
c) It has no effect on the arteries
d) It decreases the risk of arterial dissection
e) It improves arterial elasticity
8. Which study reported the highest incidence rate of vertebrobasilar stroke (VBS) related to cervical manipulation?
a) Maigne (1972)
b) Cyriax (1978)
c) Boyle et al.
d) Hosek et al. (1981)
e) Rivet and Milburn
9. Which risk factor is associated with an increased risk of cervical artery dissection?
a) A family history of migraine
b) Regular aerobic exercise
c) Adequate hydration
d) Low cholesterol levels
e) Balanced dietary habits
10. When a positive result is obtained from a vertebrobasilar insufficiency test, what is the recommended course of action?
a) Continue with cervical manipulation as planned
b) Repeat the test to confirm results
c) Stop manipulation and refer the patient for further medical evaluation
d) Apply a different treatment approach immediately
e) Monitor the patient without further action
Answers
- b) Impaired blood flow to the posterior regions of the brain
- c) C1-C2
- c) A low overall risk with considerable variability
- a) Double vision and blurred vision
- e) Joint pain in the knees
- b) To assess the integrity of vertebral and basilar blood supply
- b) It can place mechanical stress on the arteries
- c) Boyle et al.
- a) A family history of migraine
- c) Stop manipulation and refer the patient for further medical evaluation
References
- W‐L Chen, C‐H Chern, Y‐L Wu, and C‐H Lee, Emerg Med J. 2006 Jan; 23(1)Vertebral artery dissection and cerebellar infarction following chiropractic manipulation
- Assendelft W J J, Bouter L M, Knipschild P G. Complications of spinal manipulations: a comprehensive review of the literature. J Fam Pract 199642475–480. [PubMed] [Google Scholar]
- Rothwell D M, Bondy S J, Williams J I. Chiropractic manipulation and stroke. A population‐based case‐control study. Stroke 2001321054–1060. [PubMed] [Google Scholar]
- Meeker W C, Haldeman S. Chiropractic: a profession at the crossroads of mainstream and alternative medicine. Ann Intern Med 2002136216–227. [PubMed] [Google Scholar]
- Rivett DA, Milburn PA. A prospective study of cervical spine manipulation. J Man Med 1996;4:166–70.
- Boyle E, Cote P, Grier AR, et al. Examining vertebrobasilar artery stroke in two Canadian provinces. Spine 2008;33(4S):S170–
- Patijn J. Complications in manual medicine: A review of the literature. J Man Med 1991;6: 89–92.





")










")

{kind=link}