

Cervico-Thoracic Tendinitis : The Hidden Risks of Self-Adjustments
Cracking your neck or upper back can provide immediate relief… but at what cost? Behind this now-common gesture, often repeated several times a day, lies a veritable biomechanical trap. By mobilizing the wrong areas—often hypermobile or compensatory—the body enters a vicious cycle of muscle tension, joint imbalances, and, ultimately, chronic tendonitis.
The cervical and thoracic muscles, on the front line, undergo progressive overload, often ignored until the pain sets in permanently. In this article, we explore the long-term effects of self-adjustments, the warning signs, and the sustainable solutions offered by osteopathy to break this spiral.
When relief becomes overwork: a contextualization of self-adjustments
In a world where self-care is increasingly valued, it’s no surprise to see the rise in popularity of self-adjustment practices, particularly for the neck and back. Cracking one’s vertebrae is becoming, for many, an almost daily ritual. Immediate relief, temporary relaxation, the feeling of having “put something back in place”—there are so many reasons why people repeat these actions, often without realizing the consequences.
But behind this apparent liberation lies a much more complex mechanism. What appears to be liberating in the short term can, in the medium or long term, lead to insidious imbalances in the body. Because repeated adjustment of a joint is not neutral: it engages the soft tissues, ligaments, fascia, and especially the muscles surrounding the manipulated area. And these muscles, subjected to repeated mechanical constraints, sometimes enter a cycle of overuse that can lead to chronic tendonitis, persistent pain, or more general postural disorders.
The cervical region is particularly affected. Richly innervated, constantly used to stabilize the gaze and accompany head movements, it is also vulnerable to microtrauma. When we manipulate this region without precise knowledge of the primary joint fixations—those areas which, when restricted, lead to compensations elsewhere—we risk mobilizing only secondary areas, often already hypermobile. The result? Hypermobilization of certain vertebrae, joint instability, and above all, overloading of the muscle groups that are trying, as best they can, to maintain balance.

The cervical and thoracic muscles, on the front line, then become the silent victims of this habit. The upper trapezius, scalenes, suboccipitals, and thoracic paravertebrals all participate in the permanent postural adjustment of the trunk and spine. When these muscles are repeatedly stressed by inappropriate self-manipulation gestures, they contract defensively, become inflamed, and can develop repeated tendon injuries. These micro-lesions, often ignored at first, develop into painful tendonitis, persistent sensations of tension, or even radiation in the arms or between the shoulder blades.
Added to this purely biomechanical logic is a behavioral aspect. In a context of stress, mental overload, or anxiety, the urge to “crack” one’s neck can become compulsive. The gesture becomes an outlet, a way to reconnect with one’s body, or to regain some semblance of control. However, this relief is often fleeting and does not address the root cause of the tension. It diverts attention from the real problem: a persistent dysfunction, an unbalanced posture, or a poorly resolved muscular constraint.
In this article, we will explore in detail the consequences of these repeated self-adjustments on the cervical and thoracic muscles, highlighting the mechanisms of overuse, the clinical signs to watch for, and the alternative solutions offered by osteopathy. Because while it is legitimate to seek to relieve your body, you still need to know how to do so without exhausting it.
Understanding the Self-Adjustment Reflex: Between Relief and Illusion
The phenomenon of joint self-adjustment—often perceived as a harmless act—deserves more critical attention. For many people, “cracking” their neck or back has become a reflexive action, often associated with a form of bodily liberation. But what’s really at play behind this reflex? Why does this need recur so often, and what mechanisms are actually involved?

A noticeable, but deceptive, relief
The first thing to understand is the immediate relief provided by a joint crack. This is the result of several factors: the release of a gas (often carbon dioxide or nitrogen) into the joint during the rapid separation of the articular surfaces, the stimulation of local mechanical receptors, and the transient change in pain perception via ascending neurological pathways.
This phenomenon generates a feeling of immediate relaxation , often reinforced by a change in local proprioception (the brain perceives a more “mobile,” more “free” area). But this sensation is illusory if it does not correspond to a real correction of a primary restriction. In most cases, it is hypermobile or compensatory areas that are manipulated, which produces a temporary effect, but which disrupts the body’s mechanical balance in the long term.

A gesture that quickly becomes compulsive
In some people, joint cracking becomes a compulsive behavior . This is explained by several psychoneurophysiological mechanisms:
- The crunch triggers a mini-dopamine rush , reinforcing the feeling of immediate gratification.
- It helps to divert attention from internal discomfort, creating an avoidance mechanism.
- It responds to a need for body control in times of stress or anxiety.
Thus, a vicious circle appears : tension > self-adjustment > temporary relief > return of tension (often worsened) > new cracking.
This pattern can lead to a loss of proprioceptive cues , as the brain becomes accustomed to a constant state of tension and reacts with inadequate release strategies.

Sometimes aggressive and poorly targeted gestures
Most self-adjustments are performed without knowledge of the actual mechanical axes of the vertebral joints . Sudden twists or flexions are applied, often with exaggerated amplitude and uncontrolled speed. Unlike a manual adjustment performed by an osteopath or chiropractor, which aims for precise joint fixation , self-adjustment acts in a diffuse manner , affecting secondary structures and sometimes even causing micro-traumas.
For example, repeated manipulation of the upper cervical region can irritate the suboccipital muscles and nearby nerves, leading to headaches, dizziness, or eye strain.
When illusion turns into chronic tension
The paradox is that the more we seek relief through repeated adjustments, the more the body settles into a state of muscular alert . The muscles, overused to compensate for the effects of these gestures, enter a state of defensive contraction , sometimes with the appearance of myofascial trigger points . These tensions are no longer only linked to the initial cause, but become self-sustained by the self-adjustment behavior itself .
Primary vs. Secondary Fixations: Understanding the Real Areas to Correct
One of the most common mistakes made during self-adjustments is to mobilize a joint that “cracks easily,” without realizing that this is often secondary to the overall dysfunction. To fully understand why this type of manipulation can worsen the situation in the long term, we must return to an essential distinction in osteopathy: that between primary fixation and secondary fixation.

Primary fixation: the heart of imbalance
A primary fixation refers to a restriction of mobility of a tissue or joint that plays a causal role in the mechanical imbalance of a segment or body system. It is not always painful or perceptible to the patient. It may reside in a limited mobility joint, a poorly positioned organ, long-standing fascial tension, or a point of restriction linked to past trauma.
What characterizes a primary fixation is that it leads to remote compensations . The body organizes itself around this node of tension to maintain a functional balance, even if it means over-stressing other structures. These compensatory zones, in an attempt to help, become more mobile, more active, but also more vulnerable.
Secondary fixation: the compensation that attracts attention
A secondary fixation , on the other hand, is often the area that gets the most attention : the one that pulls, that blocks, that cracks. But it is only the consequence of a deeper problem. These areas appear restricted on examination, but their tension is reflexive, adaptive, defensive.
These are often the ones that are manipulated by mistake, because they give the illusion of a mechanical problem, when in reality, they are protecting another area. By mobilizing these structures too often, we weaken their capacity for compensation , we increase their hypermobility, and we risk causing inflammatory or tendon disorders.
Why Self-Adjustment Almost Always Targets the Wrong Area
The spontaneous gesture of self-adjustment generally targets an area that is easy to mobilize , accessible by hand or by a twisting movement. We hear a “crack”, we feel a release… but we have just released a secondary fixation , often already stressed or overused. It is a bit like trying to stabilize a wobbly table by unscrewing the compensating leg even more.
The illusion of well-being masks a disorganization of proprioception : the brain believes the problem is solved, while it silently worsens. The primary fixation, however, remains there, always inactive, always dysfunctional.
The osteopathic approach: looking for the cause, not the effect
This is where the osteopath’s role takes on its full meaning. Through fine palpation, analysis of tension chains, and understanding bodily compensations, the therapist is able to get to the source of the imbalance. He doesn’t just release what’s blocking things; he identifies what’s generating the tension.
Targeted release of a primary fixation often allows several secondary areas to spontaneously release. This is the whole logic of indirect treatments, functional techniques, or certain cranial approaches: work less hard, but more accurately.
Biomechanical mechanisms of muscle overuse
When we repeatedly self-adjust, especially indiscriminately, we disrupt a delicate balance between joint, ligament, and muscle structures. This imbalance can lead to chronic overuse of postural muscles, particularly in the neck and upper back. It’s not so much the movement itself that’s problematic, but its repetition in inappropriate areas, combined with the lack of recovery and neuromuscular regulation.
Reflex hypertonia and segmental protection
When an individual cracks their neck or back inappropriately, they stimulate areas that are often already hypermobile or unstable . To prevent a loss of stability, the body mounts a reflex response: the stabilizing muscles contract defensively . This is called reflex hypertonia .
This involuntary contraction is a protective mechanism which, if repeated, becomes chronic . The muscle no longer returns to its normal resting state. It remains overactivated , as if on permanent standby, ready to compensate. In the long term, this defensive posture leads to muscle shortening, a loss of flexibility and a reduction in local joint range of motion.
Repetitive Strain Injuries: The Path to Tendonitis
A permanently contracted muscle is a poorly irrigated muscle . Its vascularization becomes deficient, the elimination of metabolic waste slows down, and the connective tissues surrounding it (tendon, sheath, fascia) become more rigid and more vulnerable. If we continue to repeat self-adjustment gestures without releasing the primary fixation or relaxing the compensations, we cause a series of microtraumas in the muscle and tendon fibers.
This can lead to:
- Deep, poorly localized, dull or burning pain;
- The appearance of tendonitis , particularly in the deep cervical muscles (scalenes, levator scapula, suboccipitals);
- A drop in functional performance , with rapid fatigue of the affected muscles.
Proprioceptive disorganization and functional vicious circle
The proprioceptive system, which allows the body to locate itself in space and finely regulate its movements, depends largely on the quality of the afferents coming from the muscles and joints . When we regularly force mobilizations on unstable areas, the proprioceptive signals become incoherent : the brain receives paradoxical information, which disrupts motor regulation.
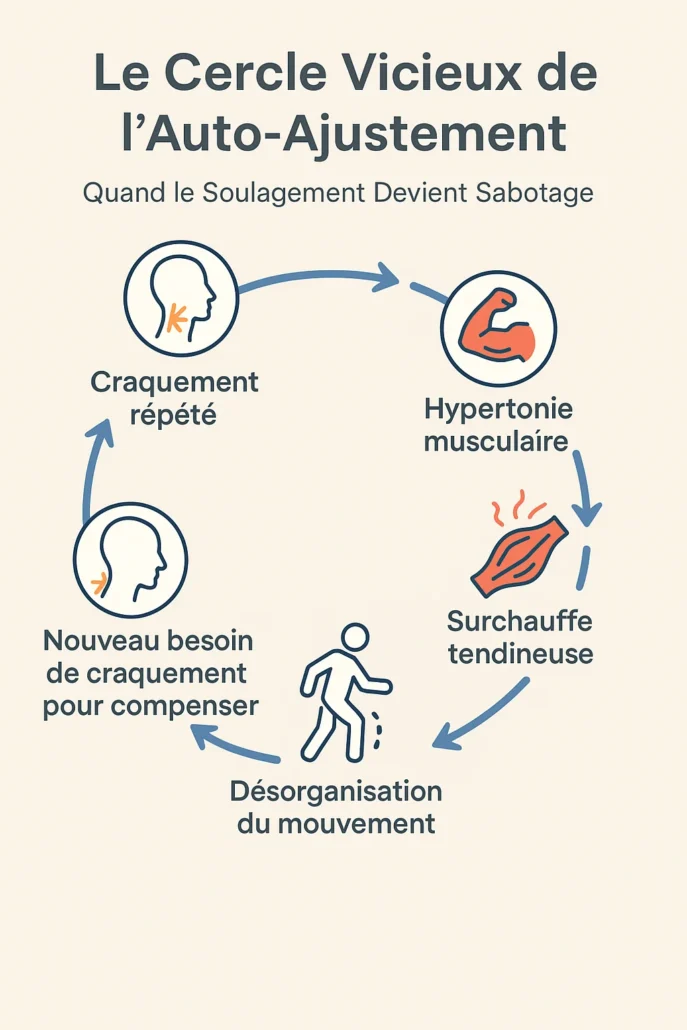
The body then enters a vicious circle :
- Repeated cracking ➝
- Muscle hypertonia ➝
- Tendon overheating ➝
- Disorganization of movement ➝
- New need for crunching to compensate.
This pattern can lead, in the medium term, to more global disorders: postural imbalances, chronic pain, cervicogenic vertigo, or persistent interscapular tension.
Consequences on muscle chains
The cervical and thoracic spine do not function in isolation. The tensions induced by self-adjustments spread to the longitudinal muscle chains , in particular:
- The posterior chain: connecting the suboccipitals, the cervical and thoracic paravertebrals, the quadratus lumborum, up to the hamstrings.
- The anterolateral chain: including the scalenes, diaphragm, psoas, and intercostal muscles.
Therefore, poorly managed cervical dysfunction can cause downward repercussions , such as lower back pain or respiratory problems of muscular origin.
Biomechanical mechanisms of muscle overuse
The neck is a fascinatingly complex anatomical region. Its remarkable mobility allows for a wide range of movements: rotation, flexion, extension, and tilt. But this flexibility comes at a price. The cervical muscles work constantly to stabilize the head and compensate for micro-movements of the trunk. When they are disrupted by repeated self-adjusting movements, they quickly become the silent victims of chronic overuse.
Suboccipital: tension, migraines and dizziness

Located between the base of the skull and the first cervical vertebra, the suboccipital muscles are small but essential. Their main role is to stabilize fine head movements and adjust gaze.
When this region is frequently manipulated (often by “cracking” the upper neck in rapid extension or rotation), these muscles become hypertonic , irritated, or even inflamed. We then observe:
- headaches of cervical origin (particularly helmet or occipital band headaches),
- visual or concentration problems ,
- a feeling of dizziness or unsteadiness , especially when sitting for long periods.
These signs can easily be confused with other pathologies, while they are often due to poor management of local tension.
Scalenes: forced stretching and radiating tension

The scalene muscles , located on the sides of the neck, play an important role in breathing (they elevate the first ribs) and in lateral stabilization of the cervical spine.
Repeated manipulations that involve excessive lateral tilts or rotations put these muscles into repetitive passive stretching , which creates:
- chronic muscle fatigue ,
- painful trigger points , radiating to the arm or chest,
- a risk of thoracic outlet syndrome , if the scalenes compress the nerves of the brachial plexus.
Many patients with shoulder or arm pain actually have an underestimated cervical origin.
Scapula levator: a muscle under constant overload

Attached to the scapula and cervical vertebrae C1 to C4, the levator scapulae is constantly recruited to keep the shoulders balanced. In cases of stress, closed posture or cervical tension, it often becomes the site of chronic unilateral pain , especially on the dominant side.
In people who frequently manipulate their neck by pulling the head towards the shoulder or by “pushing” by leverage, this muscle is in prolonged eccentric contraction , promoting:
- painful local tensions ,
- a restriction of cervical rotation ,
- compensatory overload of the upper trapezius muscles.
Other muscles impacted and domino effect
Although the suboccipitals, scalenes, and levator scapulae are most commonly affected, other muscles contribute to the overall imbalance:
- Longus colli : deep muscle essential for anterior cervical stability, often inhibited in postural compensations.
- Upper trapezius : already over-recruited by stress, it readily compensates for a loss of cervical mobility.
- Cervical paravertebral : often stretched asymmetrically, generating a permanent rotation of the neck not perceived by the patient.
These tensions are not isolated. They interact within a broader postural network, affecting the shoulders, thorax, and even the pelvis in chronic patients.
Biomechanical mechanisms of muscle overuse
While the cervical regions are the first to be affected by self-adjustments, the upper thoracic and interscapular areas are not left out. Many patients describe sensations of blocking between the shoulder blades, diffuse discomfort in the upper back, or even an irresistible urge to “crack” their thoracic spine by pushing their torso against a chair or table. These actions, although instinctive, can lead to chronic overload of certain deep postural muscles , essential for the stability of the rib cage and shoulder girdle.
Rhomboids and middle trapezius: the muscles of interscapular “pulling”
The rhomboids (minor and major) and the middle trapezius connect the thoracic vertebrae to the scapula. They stabilize the scapula and allow its coordinated movement during arm movements.

When we try to self-manipulate our upper back by arching or forcing a thoracic rotation (often while sitting), these muscles are stretched abruptly , especially if they are already tense. This triggers a series of reactions:
- Repeated myotendinous microtrauma ;
- Chronic interscapular pain , often confused with pulmonary or cardiac pain;
- Disorganization of scapulothoracic coordination , with long-term fatigue.

This phenomenon is amplified in people with a curled posture (thoracic kyphosis, office work, chronic postural stress).
Thoracic paravertebrals: the ignored stabilizers
The thoracic erector spinae muscles (spinalis, longissimus, iliocostalis) are smaller than their lumbar counterparts, but play a crucial role in trunk stability . When you try to cause extension or “unlocking” by pushing your back backward, these muscles take the load.
In the long term:
- They develop chronic hypertonia , especially between T4 and T8;
- Their costal insertions become sensitive, generating diffuse thoracic pain, sometimes interpreted as visceral pain (reflux, chest tightness);
- They become ineffective in their stabilizing role , accentuating mechanical instability.
Serratus posterior superior and intercostals: the forgotten ones in the respiratory gesture
Often overlooked, the intercostal muscles and serratus posterior superior are essential for respiratory dynamics. In cases of repeated thoracic self-adjustment, these muscles are mobilized in sudden movements , which creates paradoxical fatigue.
We then observe:
- Less ample breathing , compensated by cervical accessory muscles;
- A sensation of costal blockage , with localized pain on deep inspiration;
- A fixed posture in rigid kyphosis , due to the loss of segmental and muscular mobility.
Link with overall posture: between fatigue and locking
These thoracic muscle over-stresses do not remain local. They influence:
- General posture of the trunk , with loss of mobility of the shoulders and neck;
- The breathing pattern , which becomes rigid, promoting anxiety and chronic fatigue;
- Lower compensation mechanisms , particularly at the lumbar or diaphragm level.
People who regularly “crack” their backs often develop defensive postural locking mechanisms . Their trunk becomes less fluid, less coordinated. Each attempt at joint release increases muscle tension, creating a breeding ground for tendonitis, contracture, or neuromuscular exhaustion.
Clinical Case Studies: When Crack Becomes Chronic
The harmful consequences of repetitive self-adjustments are not just theoretical: they are observed every week in the practice. Chronic pain, functional limitations, recurrent tendonitis… These symptoms often originate not from a sudden trauma, but from gestural behavior that has become routine , sometimes even unconscious. Here are two typical cases encountered in osteopathy, representative of this mechanism of muscular exhaustion.
Case 1: The daily cervical cracking ritual
Patient profile:
34-year-old female executive working from home, chronic stress, prolonged screen time.
Reason for consultation:
Frequent headaches at the end of the day, neck/upper back tension, occasional dizziness.
Reported behavior:
Self-manipulation of the neck 4 to 6 times a day: lateral grip of the head with rapid twisting of the cervical spine. Immediate feeling of relief, but pain that always returns to the same place.
Osteopathic assessment:
- Hypertonia of the suboccipital and scalene muscles.
- C1-C2 joint hypermobility with fixation of C5-C6.
- Inhibition of the deep cervical muscles (long neck).
- Cervical trigger points with radiation to the temples.
Analysis:
The patient constantly manipulates the reacting region (C1-C2) but does not address the structural cause (lower fixation + postural disorganization). The brain interprets the relaxation as a resolution, reinforcing addictive behavior , without resolving the restriction.
Proposed treatment:
- Deep myofascial work on the suboccipital muscles.
- Indirect techniques to release C5-C6.
- Cervical centering exercises (proprioception + stabilization).
- Gradual weaning from self-adjustments + conscious breathing.
Progression at 3 weeks:
70% reduction in headaches. Dizziness disappeared. Patient surprised by the spontaneous return of mobility after abandoning the “reflex cracking”.
Case 2: The back that “blocks” at work
Patient profile:
42-year-old male, skilled worker, physical labor, heavy lifting.
Reason for consultation:
Chronic interscapular pain, need to “crack” the upper back by leaning against a chair. Pain with deep breathing and trunk extension.
Reported behavior:
Arches against armrests or hard backrest 4-5 times a day to get a chest “click.”
Osteopathic assessment:
- Hypertonia of the rhomboids and middle trapezius.
- Bilateral trigger points with costal irradiation.
- Fixation of T4-T6 segments (thoracic hinge area).
- Upper costal shallow breathing.
Analysis:
The patient manipulates an already overstressed unstable area (T3-T5), which aggravates local tension. Thoracic segmental fixation is never addressed. The compensatory muscles are overheated , without recovery.
Proposed treatment:
- Gentle decompression of the thoracic hinge.
- Release of intercostal fascia.
- Diaphragmatic work and postural opening.
- Education in conscious movement and interscapular strengthening.
Progression at 1 month:
Clear reduction in the frequency of pain, improvement in breathing pattern, end of induced cracking. Sensation of more “vertical” posture and more ample breathing.
Case 3: Daily cervical self-manipulations and chronic headaches
Patient profile : Female, 33 years old, executive working from home, occasional sportswoman.
Habit : Daily cervical mobilization, sometimes several times an hour, in forced rotation.
Reason for consultation : Occipital band headaches, morning stiffness, occasional dizziness.
Osteopathic assessment :
- Marked hypertonia of the suboccipitals , scalenes and levator scapula .
- Hypermobility of C1-C2, with lower fixation (C5-C6).
- Presence of active trigger points radiating to the temporal region.
Interpretation :
The relief perceived after each crack is related to the stimulation of hypermobile areas, but the primary (lower) fixation remains uncorrected. The maintenance of muscle hypertonia increases headaches, creating a self-perpetuating loop.
Support :
- Gentle C5-C6 decompression techniques.
- Suboccipital myofascial work.
- Postural education and self-regulation exercises (breathing, proprioception).
- Recommendation: Complete cessation of self-manipulation for 3 weeks.
Case 4: Interscapular pain and postural overexertion syndrome
Patient profile : Male, 41 years old, programmer, history of mild scoliosis.
Habit : Back pressure against a rigid backrest to “unlock” the shoulder blades several times a day.
Reason for consultation : Dull, persistent pain between the shoulder blades, with a sensation of chest “locking”.
Osteopathic assessment :
- Marked tension in the rhomboids and middle trapezius .
- Loss of mobility between T4-T8.
- Scapular compensation, with chronic elevation and internal rotation of the scapulae.
Interpretation :
Thoracic self-adjustments engage stabilizing muscles without correcting the loss of deep segmental mobility. Result: muscle overload , myotendinous fatigue, and impaired proprioception.
Support :
- Soft segmental treatment on the T4-T8 hinge.
- Specific interscapular stretches.
- Light postural strengthening (e.g. serratus anterior, deep lumbar muscles).
- Learning gentle self-mobilizations in controlled thoracic rotation.
Case 5: Cervicothoracic self-adjustments and diffuse pain
Patient Profile : 26-year-old osteopathy student with chronic stress and sleep disturbances.
Habit : Frequent neck and upper back cracking during revision.
Reason for Consultation : Fluctuating neck and upper back pain and chronic fatigue.
Osteopathic assessment :
- Dysfunction of the cervicothoracic junction.
- Hypertonia of the upper trapezius , long neck inhibited.
- Respiratory dysrhythmia with excessive chest elevation.
Interpretation :
The need to crack is linked to an attempt at emotional release and sensory discharge. Autonomic dysregulation increases muscular tension and accentuates the use of reflexive gestures.
Support :
- Global tissue approach (fascia, diaphragm, skull base).
- Neurovegetative rebalancing (cranial work, guided breathing).
- Implementation of postural relaxation rituals.
Osteopathic approach: breaking out of the cycle of tension
Faced with the harmful effects of repeated self-adjustments, osteopathy offers a gentle, targeted alternative that is deeply respectful of the body’s intelligence. Far from forcing or “unblocking” at all costs, the osteopathic practitioner seeks to understand the origin of the imbalance , to restore primary mobility , and to reduce unnecessary muscular over-stress . It is not just a matter of treating a symptom, but of putting the body back into a logic of sustainable self-regulation .
1. Identify the primary fixation: the heart of the approach
The first step in osteopathic treatment is to identify the true source of the dysfunction . This requires careful listening to the body, precise palpation, and a comprehensive vision. It is not simply a matter of manipulating the painful area, but of finding the first restriction that led to a whole cascade of compensations.
For example :
- Loss of mobility between C5 and C6 can lead to hypermobility at C1-C2, often cracked in self-adjustment.
- Diaphragmatic fascial tension can generate hypertonia of the scalenes or intercostal muscles.
- An old abdominal scar can disrupt the myofascial chains and induce cervical or dorsal overload.
It is by releasing this primary cause that we allow the rest of the body to relax spontaneously and deeply.
2. Release without rushing: adapted techniques
The osteopath has a wide range of techniques , which he adapts according to the patient, his age, his sensitivity and his level of chronicity. In the case of tensions linked to self-adjustments, the following techniques are often preferred:
- Functional and indirect techniques : which respect the natural movement of the body, ideal for hypermobile or painful areas.
- Myotensive techniques : to help a hypertonic muscle relax without sudden stretching.
- Cranial and visceral techniques : to reharmonize deep tensions and autonomous regulation systems.
- Recoil and tissue listening techniques : to revive the vitality and natural elasticity of tissues.
The goal is not to “make noise,” but to restore lasting balance to the body structure.
3. Restore proprioception and body schema
Once the main tensions have been released, it is essential to retrain the body’s perception of space. The brain must find reliable reference points to avoid falling back into harmful automatisms of self-manipulation.
This involves:
- Body awareness exercises ( e.g. micro-movements, postural anchoring, directed stretching).
- Gentle mobilizations to do at home , focused on breathing and fine mobility.
- Sensorimotor reprogramming , sometimes in conjunction with a physiotherapist or a functional movement coach.
The patient becomes an actor in their rebalancing , which reinforces the effectiveness of the treatment.
4. Reestablish a healthy relationship with the body
Osteopathy also acts on a more symbolic and emotional level. Cracking one’s neck can be an expression of a need for control, emotional relief, or anchoring in a body perceived as tense or unstable. The osteopathic approach, through respectful touch, holistic listening, and regulation of the autonomic nervous system, often allows the patient to regain a more peaceful relationship with their body .
Practical tips and alternatives to self-adjustments
Rather than repeatedly cracking your back or neck, there are safer, longer-lasting, and often more effective strategies for relieving tension , restoring mobility, and regaining control of your bodily comfort . This section presents simple, accessible, and physiologically sound approaches to incorporate into your daily routine.
1. Gentle self-mobilizations: controlled movements, without cracking
Self-mobilizations differ fundamentally from self-adjustments: they aim to restore joint mobility without forcing, while respecting the natural limits of the tissues.
Some examples:
- Slow tilts of the head , following the axis of the shoulders, without jolts;
- Progressive cervical rotations , in synchronization with breathing;
- Seated thoracic flexions and extensions , on a ball or against a wall, seeking relaxation and not tension;
- Trunk rotations with arms crossed over the shoulders, while inhaling deeply, to promote costal mobilization.
Objective: to restore movement to the joint system while recalibrating the proprioceptive sensors , without triggering a muscular defense reflex.
2. Neuromotor and self-rehabilitation exercises
The idea here is to retrain the muscular and nervous system to function in synergy, without over-stressing.
Some ideas:
- Eye-head-trunk coordination exercises , to recalibrate the cervicothoracic junction (e.g.: following a target with the eyes and turning the head in opposition);
- Postural stabilization on an unstable surface (proprioceptive cushion) in a sitting or standing position;
- Targeted strengthening of deep stabilizing muscles: long neck, cervical multifidus, deep interscapular muscles;
- Work on controlled breathing (cardiac coherence, slow costal or diaphragmatic breathing) to unlock muscle chains under chronic tension.
These exercises should be adapted with a therapist depending on the case, but some can be easily integrated into daily life.
3. Postural work and body awareness
A distorted body image is often the root cause of the compulsive need to crack. Re-engaging one’s body in space, through gentle practices, is a powerful and preventative strategy.
Recommended approaches:
- Alexander Method , Feldenkrais or Antigymnastics : to reconnect the brain to simple but precise movements;
- Guided self-stretching , with visualization of the movement (e.g.: “I lengthen my spine”, “my shoulders move away from my ears”);
- Active micro-relaxation : anchoring yourself in the body through small conscious movements, several times a day;
- Acupressure mats or gentle self-massage rollers , not to “crack”, but to release surface tension.
4. Know when to consult: warning signs
It’s important to know when to limit self-comfort. There are some signs that it’s time to seek professional help:
- Compulsive need to binge several times a day;
- Persistent pain despite cracking;
- Appearance of new symptoms (dizziness, numbness, intense fatigue);
- Feeling that the neck or back becomes “unstable” or “floating.”
An osteopath can then make a global assessment , redirect if necessary, and propose appropriate and progressive treatment.
Conclusion: Self-adjustment or self-sabotage?
It is human nature to seek to relieve tension, blockage, or diffuse discomfort. In a world where the body is often put to the test—by stress, a sedentary lifestyle, or awkward postures—the self-adjustment reflex appears to be a legitimate attempt to regain control. But this gesture, repeated without awareness or discernment, can become a muscular trap , perpetuating the imbalances it claims to alleviate.
In this article, we have seen how the cervical and thoracic muscles become the first silent victims of this immediate relief strategy. We have explored the biomechanical mechanisms , the reflex loops , and the possible side effects , ranging from simple discomfort to chronic tendonitis.
Osteopathy, in its global and respectful vision of the living, does not condemn the search for autonomy. On the contrary, it encourages it, but within an enlightened framework . It invites us to change our perspective: from the need to “make things crack” to the art of “letting the tissues breathe.” From the impulse to correct, to listening to a deeper imbalance.
So, should we ban all self-adjustment? Not necessarily. But above all, we need to rethink our relationship with reflexive gestures , question them, and listen to them. Behind each “crack” perhaps lies an older tension, a more deeply rooted posture, a message from the body waiting to be translated.
What if, rather than forcing things, we learned to dialogue with our tensions?
Scientific and clinical references
- Evans, D. W. (2002). Mechanisms and effects of spinal high-velocity, low-amplitude thrust manipulation: a comprehensive review. Manual Therapy, 7(2), 94–102.
https://doi.org/10.1054/math.2001.0407
Comprehensive analysis of the biomechanical and neurophysiological effects of spinal manipulation.
- Haavik, H., & Murphy, B. (2012). The role of spinal manipulation in addressing disordered sensorimotor integration and altered motor control. Journal of Electromyography and Kinesiology, 22(5), 768–776.
https://doi.org/10.1016/j.jelekin.2012.02.012
Shows how adjustments can change body perception and motor skills.
- Fernandez-de-Las-Penas, C. et al. (2006). Myofascial trigger points in subjects presenting with mechanical neck pain: a blinded, controlled study. Manual Therapy, 12(1), 29–33.
https://doi.org/10.1016/j.math.2006.02.002
Provides strong evidence for the involvement of trigger points in neck pain.
- Chaitow, L., & DeLany, J. W. (2011). Clinical Application of Neuromuscular Techniques: Volume 1, The Upper Body. Churchill Livingstone.
Reference work on the management of chronic muscle tension, very useful for understanding tissue responses to manipulation.
- Scali, F., Pontell, M. E., & Enix, D. E. (2013). Histological analysis of human upper cervical ligaments. Journal of Chiropractic Medicine, 12(1), 15–20.
https://doi.org/10.1016/j.jcm.2012.11.001
Provides an overview of structures sensitive to hypermobilization in the C0–C2 region.
- O’Sullivan, P. B. (2005). Diagnosis and classification of chronic low back pain disorders: maladaptive movement and motor control impairments as underlying mechanism. Manual Therapy, 10(4), 242–255.
https://doi.org/10.1016/j.math.2005.07.001
Applicable to the cervical and thoracic spine in terms of motor control.
- Simons, D. G., Travell, J. G., & Simons, L. S. (1999). Travell & Simons’ Myofascial Pain and Dysfunction: The Trigger Point Manual. Vol. 1.
Fundamental work for understanding muscle pain secondary to joint dysfunction.
- Bron, C., Dommerholt, J., & Stegenga, B. (2008). High prevalence of shoulder girdle muscles with myofascial trigger points in patients with shoulder pain. BMC Musculoskeletal Disorders, 9(1), 139.
https://doi.org/10.1186/1471-2474-9-139
Highlights secondary muscle compensations in scapular disorders.
- Jull, G., & Falla, D. (2016). Dysfunction in the cervical musculature: assessment and clinical implications. In Grieve’s Modern Musculoskeletal Physiotherapy (4th ed.).
Essential chapter for clinicians treating chronic cervicothoracic tension.









{kind=link}