

Introduction
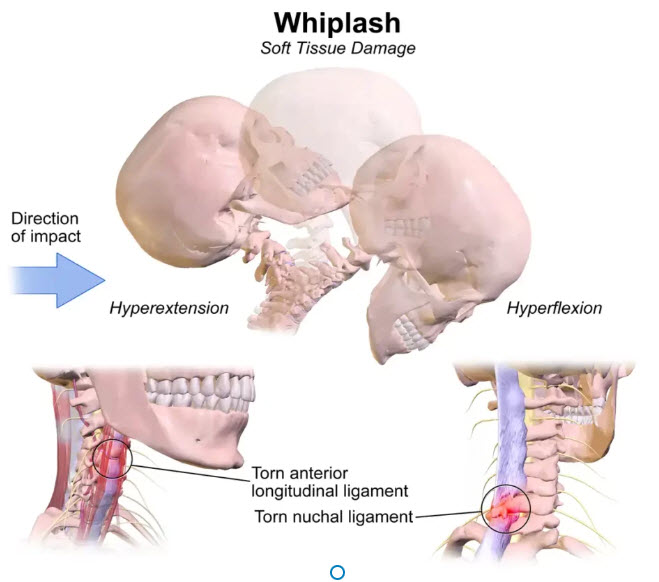
Le coup de fouet cervical, également connu sous le nom de traumatisme cervical accéléré, est une blessure courante qui survient souvent lors d’accidents de voiture, en particulier lors de collisions arrière. Cette condition se produit lorsque la tête est brusquement projetée en arrière puis en avant, créant une force hyperextension et hyperflexion sur la colonne cervicale.
Les symptômes du coup de fouet cervical peuvent varier en intensité et en durée. Dans de nombreux cas, les symptômes se manifestent quelques heures à quelques jours après l’accident. Les patients peuvent ressentir une raideur au niveau du cou, des maux de tête, des vertiges, des troubles de la mémoire, des troubles du sommeil et parfois des douleurs irradiant vers les épaules et le dos.
Il est essentiel de prendre en compte non seulement les symptômes physiques, mais aussi les aspects émotionnels liés à l’accident. Certains patients peuvent développer de l’anxiété ou des troubles du sommeil en raison du traumatisme subi.
En ce qui concerne la prévention, l’éducation des patients est cruciale. Conseillez-leur sur l’importance de porter correctement la ceinture de sécurité, de régler correctement les appuie-tête et de maintenir une posture appropriée tout en conduisant. Des exercices de renforcement musculaire peuvent également être recommandés pour renforcer la stabilité de la région cervicale.
Un facteur contributif à l’accident lui-même peut résider dans l’activation de points déclencheurs au sein de la division claviculaire du muscle sternocléidomastoïdien. Ces points déclencheurs peuvent induire des vertiges lorsqu’une personne tourne rapidement la tête, comme cela peut se produire lors d’un examen des épaules tout en conduisant. Ces vertiges présentent un risque potentiel, car ils peuvent entraîner une perte de contrôle du véhicule par le conducteur (Travel, Simons, 1983). La vitesse des véhicules impliqués dans l’accident ou l’ampleur des dommages physiques subis par le véhicule peuvent ne pas être directement liées à la gravité des blessures cervicales.
Des vitesses aussi modestes que 15 miles à l’heure peuvent générer suffisamment d’énergie pour déclencher un coup du fouet cervical chez les occupants, même lorsqu’ils portent une ceinture de sécurité. Parmi les autres causes fréquentes du coup du lapin, citons les blessures par contact, les impacts à la tête dus à la chute d’objets ou à des agressions. Les tensions cervicales résultant de brusques changements de direction, tels que des montagnes russes, des accidents mineurs à vélo, des chutes et des glissades, peuvent toutes entraîner un coup du fouet cervical.

Les traumatismes liés au stress répétitif ou aux tensions chroniques impliquant le cou, tels que l’utilisation du cou pour tenir un téléphone, constituent des causes fréquentes mais non aiguës. Les mauvais traitements envers les enfants, en particulier l’agitation d’un enfant, peuvent également provoquer cette blessure, ainsi que des lésions plus graves au niveau du cerveau ou de la colonne vertébrale de l’enfant.
Le cartilage situé entre le disque intervertébral et l’os vertébral est fréquemment sujet à des fissures, constituant ainsi ce que l’on appelle une lésion du rebord. Les dommages infligés au disque peuvent exercer une pression sur les nerfs lors de leur émergence de la colonne vertébrale. Cette pression ou irritation peut se manifester par des symptômes tels que l’engourdissement de la peau, une faiblesse musculaire ou une douleur suivant le trajet du nerf.
La plupart des gens associent ces symptômes à un nerf pincé (radiculopathie cervicale). Les tissus mous entourant l’articulation de la facette peuvent également subir des blessures, car de nombreux nerfs sensibles de la colonne vertébrale sont situés au niveau de ces articulations. Les surfaces normalement lisses sur lesquelles ces articulations glissent peuvent devenir rugueuses, irritées et enflammées. Des recherches démontrent que la douleur au niveau du cou provient fréquemment de l’altération des articulations des facettes. La lombalgie est souvent observée comme une caractéristique courante après une blessure au coup du fouet cervical.
Des études indiquent qu’une activité électrique significative se produit dans les muscles de la colonne lombaire lors de l’extension du cou. Cette réaction s’intensifie en présence de douleurs cervicales, peut-être comme un moyen de stabiliser la colonne vertébrale face à une faiblesse causée par la douleur au cou. Les muscles du cou réagissent de manière particulièrement sensible aux changements soudains de tension, avec de minuscules fuseaux musculaires signalant la nécessité d’une tension accrue pour contrer des mouvements brusques. Il en résulte souvent des spasmes musculaires en tant que mécanisme d’autoprotection. Ce renforcement du tonus musculaire limite le mouvement de l’articulation enflammée, pouvant entraîner une raideur au niveau de la nuque.
Causes
Les coups de fouet cervical, également connus sous le nom de coup du lapin, sont souvent déclenchés par des mouvements brusques du cou, principalement d’avant en arrière. Ces incidents surviennent fréquemment lors d’accidents de voiture, de chutes ou de collisions sportives. Les causes des coups de fouet cervical sont profondément liées à la manière dont le cou réagit à des forces soudaines et inattendues. Lors d’un accident de voiture, par exemple, la rapidité avec laquelle le véhicule s’arrête peut provoquer un mouvement brusque du cou, mettant à rude épreuve les muscles, ligaments et tendons. De même, lors de certaines activités sportives, les impacts violents peuvent entraîner un déséquilibre et des contraintes excessives sur la région cervicale.
Introduction
Whiplash, also known as accelerated whiplash injury, is a common injury that often occurs in car accidents, particularly in rear-end collisions. This condition occurs when the head is abruptly thrown backward and then forward, creating a hyperextension and hyperflexion force on the cervical spine.
Whiplash symptoms can vary in intensity and duration. In many cases, symptoms appear a few hours to a few days after the accident. Patients may experience neck stiffness, headaches, dizziness, memory problems, trouble sleeping, and sometimes pain radiating to the shoulders and back.
It is essential to take into account not only the physical symptoms, but also the emotional aspects related to the accident. Some patients may develop anxiety or sleep problems due to the trauma they experienced.
When it comes to prevention, patient education is crucial. Advise them on the importance of wearing seat belts correctly, adjusting head restraints correctly, and maintaining proper posture while driving. Muscle strengthening exercises may also be recommended to increase stability in the cervical region.
A contributing factor to the accident itself may lie in the activation of trigger points within the clavicular division of the sternocleidomastoid muscle. These trigger points can induce dizziness when a person turns their head quickly, as can occur when checking the shoulders while driving. This dizziness presents a potential risk, because it can cause the driver to lose control of the vehicle (Travel, Simons, 1983). The speed of the vehicles involved in the accident or the extent of physical damage to the vehicle may not be directly related to the severity of the neck injuries.
Repetitive stress or chronic strain injuries involving the neck, such as using the neck to hold a phone, are common but not acute causes. Child abuse, especially restlessness of a child, can also cause this injury, as well as more serious damage to the child’s brain or spine.
The cartilage between the intervertebral disc and the vertebral bone is frequently subject to cracks, thus constituting what is called a rim injury. Damage to the disc can put pressure on the nerves as they emerge from the spine. This pressure or irritation may manifest as symptoms such as numbness of the skin, muscle weakness, or pain along the path of the nerve.
Speeds as modest as 15 miles per hour can generate enough energy to trigger whiplash in occupants, even when wearing a seat belt. Other common causes of whiplash include contact injuries, impacts to the head from falling objects, or assaults. Neck strain resulting from sudden changes in direction, such as riding roller coasters, minor cycling accidents, falls and slips, can all lead to whiplash.
Most people associate these symptoms with a pinched nerve (cervical radiculopathy). The soft tissues surrounding the facet joint can also sustain injury, as many of the sensitive nerves of the spine are located at these joints. The normally smooth surfaces these joints slide on can become rough, irritated and inflamed. Research shows that neck pain frequently comes from damage to the facet joints. Low back pain is often observed as a common feature after a whiplash injury.
Studies indicate that significant electrical activity occurs in the muscles of the lumbar spine during neck extension. This response intensifies in the presence of neck pain, perhaps as a way to stabilize the spine in the face of weakness caused by neck pain. Neck muscles respond particularly sensitively to sudden changes in tension, with tiny muscle spindles signaling the need for increased tension to counteract sudden movements. This often results in muscle spasms as a self-protective mechanism. This strengthening of muscle tone limits the movement of the inflamed joint, which can lead to stiffness in the neck.
Causes
Whiplash, also known as whiplash, is often triggered by sudden movements of the neck, primarily back and forth. These incidents frequently occur during car accidents, falls or sports collisions. The causes of whiplash are deeply linked to how the neck responds to sudden, unexpected forces. In a car accident, for example, the speed with which the vehicle stops can cause the neck to jerk suddenly, putting strain on the muscles, ligaments and tendons. Likewise, during certain sporting activities, violent impacts can cause imbalance and excessive stress on the cervical region.
A major contributing factor to whiplash is the unpreparedness of the neck muscles to absorb the energy generated by these sudden movements. When the neck is not sufficiently toned or flexible, it becomes more vulnerable to injury. Poor daily posture can also play a crucial role. Long hours spent in front of a computer screen or frequent cell phone use can lead to constant muscle tension in the neck, increasing the risk of injury during a traumatic incident.
- Active Trigger Points in the Clavicular Division of the Sternocleidomastoid Muscle: These points can be activated during sudden head movements, such as when checking the shoulders while driving, causing dizziness which can be dangerous on the road (Travel, Simons, 1983).
- Speed of Vehicles Involved: The speed of the cars during the accident can influence the severity of neck injuries. Even at relatively low speeds, such as 15 miles per hour, the energy generated can be enough to trigger whiplash in occupants, even if they are wearing a seat belt.
- Type of Accident or Physical Damage Sustained: The extent of physical damage sustained by the vehicle or the type of accident may not be directly proportional to the intensity of the neck injuries.
- Other Common Causes of Whiplash: Common factors include contact injuries, head impacts from falling objects, or assaults. Additionally, neck strain from sudden changes in direction, such as minor cycling accidents, falls and slips, can also lead to whiplash.
- Repetitive Stress Injury or Chronic Strain: Prolonged use of the neck in everyday activities, such as holding a phone, can be a common but not acute cause of neck trauma.
- Child Abuse: A child’s agitation can cause whiplash, potentially leading to serious injury to the child’s brain or spine.
Symptoms
Symptoms associated with whiplash, also known as accelerated whiplash injury, present a range of manifestations that can have a significant impact on the daily lives of affected individuals. Immediately after the incident, most people feel stiffness in the neck area, accompanied by muscle pain that may extend toward the shoulders. This feeling of tension can progress to persistent headaches, often localized at the base of the skull, creating constant discomfort.
Commonly reported symptoms also include general fatigue and decreased ability to concentrate. These manifestations may be attributed to the body’s response to trauma, but their persistence may indicate deeper damage requiring careful medical evaluation. Additionally, some individuals experience numbness or tingling in the arms, shoulders, or even face, a sign of neurological disturbances that may result from whiplash.
It is crucial to recognize that these symptoms may not appear immediately after the accident. In many cases, they can appear with a delay, sometimes several hours or even days after the initial incident. This highlights the importance of continued health monitoring, even in the absence of immediate symptoms.
Psychological aspects should not be neglected, as people who have suffered whiplash can develop emotional responses such as anxiety and depression. Persistent pain and disruption to physical well-being can impact mental health, highlighting the need for a holistic approach to recovery. Healthcare professionals, particularly osteopaths who specialize in body structure and function, play a crucial role in the assessment and treatment of whiplash symptoms.
- Neck Pain: Pain in the cervical region is one of the most common symptoms.
- Cervical Stiffness: A feeling of stiffness or limitation of movement in the neck.
- Headaches: Headaches, often centered at the base of the skull, may be associated with cervical problems.
- Numbness or Tingling: Feelings of numbness or tingling in the neck, shoulders, arms, or hands.
- Muscle Weakness: Muscle weakness, particularly in the arms.
- Sensitivity to Touch: Some individuals may experience increased sensitivity to touch in the cervical region.
- Dizziness: Dizziness or lightheadedness may occur, especially with neck movements.
- Vision or Hearing Problems: In some cases, vision or hearing problems may be linked to neck problems.
- Noise or Crunching: Crunching noises or sensations in the neck during movements.
- Difficulty Swallowing: Certain cervical disorders can cause discomfort or difficulty swallowing.
It is essential to note that these symptoms can be the result of a variety of conditions, ranging from mild muscle strains to more serious problems, such as herniated discs or nerve damage.
Risk factors
The risk factors associated with whiplash injuries are diverse and can influence the likelihood of developing this traumatic injury. Car accidents represent one of the main risk situations, especially rear-end collisions where the car is suddenly stopped, causing a sudden neck movement. Sports accidents, such as collisions during contact games, also increase the risk of whiplash. Poor everyday posture, whether at work at a computer or using a cell phone for long periods of time, can contribute to neck muscle tension, making the area more vulnerable to injury during an incident.
The speed of the vehicle at the time of the accident is an important factor, as low-speed collisions can also cause whiplash. Additionally, incorrect car seat positioning, lack of head and neck support, and neglect of safety devices such as head restraints can worsen the consequences of an accident.
A person’s general physical condition also plays a crucial role. Well-trained and flexible neck muscles can offer some protection against injury during a sudden movement. Conversely, muscle weakness or reduced mobility can increase susceptibility to injury.
Finally, a history of neck injuries, even old ones, can increase the risk of developing persistent symptoms after another incident. It is important to note that psychological factors, such as post-traumatic stress, can also influence how a person responds to injuries and associated symptoms.
Understanding these risk factors can help raise awareness about whiplash prevention. Vigilance when driving, adopting good daily postural practices, strengthening the neck muscles and respecting safety rules, particularly when it comes to driving, are all measures that can help reduce the risk of this injury. traumatic.
- Poor Postures and Inadequate Ergonomics: Frequently adopting incorrect postures or working in inappropriate ergonomic conditions can increase tension on the cervical spine, thereby increasing the risk of injury.
- Road Accidents: Motor vehicle collisions, particularly whiplash accidents, represent a major risk, potentially leading to neck injuries.
- Risky Activities: Participating in sports or recreational activities involving sudden neck movements, such as motor sports, may increase the risk of neck injuries.
- Physically Demanding Job: Jobs that require significant physical effort, especially those involving repetitive neck movements, can contribute to the development of neck problems.
- Stress and Emotional Tension: Chronic stress and emotional tension can influence posture and increase the likelihood of developing neck disorders.
- Pre-Existing Conditions: Pre-existing medical conditions, such as cervical arthritis or structural abnormalities, can increase vulnerability to cervical problems.
- Age: Natural aging can lead to degeneration of intervertebral discs and joints, increasing the risk of neck injuries.
- Obesity: Excessive weight can put additional pressure on the cervical spine, increasing the risk of neck problems.
- Sedentary lifestyle: A sedentary lifestyle can weaken neck muscles and promote cervical stiffness.
- Smoking: Smoking can affect blood flow in the spinal discs, potentially contributing to cervical problems.
Understanding these risk factors allows preventative strategies to be put in place, whether through lifestyle modifications, ergonomic adjustments at work, or practicing methods to strengthen neck muscles and promote good posture.
Tissues involved in any whiplash
- All structures of the neck, upper chest, and head can be injured by whiplash.
- Cervical and thoracic vertebrae
- Intervertebral discs
- Articular facets
- Joint capsules
- Anterior, middle and posterior scalenes.
The muscles of mastication and the thorax, including the intercostals, posterior spinal muscles, and diaphragm, may also be affected.
Recommendations for those who have whiplash
Here are some general recommendations:
- Thorough Evaluation: Undergo a complete medical evaluation, which may include physical examinations, a detailed medical history, and imaging tests such as X-rays or MRIs.
- Collaboration with Specialists: Depending on the nature of your cervical problems, it may be necessary to consult specialists such as orthopedists, neurologists or osteopaths for additional advice.
- Informed choice: If osteopathy is being considered, choose a qualified osteopath. Discuss your symptoms, ask questions about specific treatment approaches, and make sure you understand the benefits and limitations of treatment.
- Regular Medical Follow-up: Be sure to follow your healthcare professional’s recommendations and schedule follow-up visits to assess the effectiveness of treatment.
- Self-Care and Prevention: Follow the lifestyle and exercise advice recommended by your healthcare professional to promote healing and prevent future neck problems.
- Be Cautious with Self-medication: Avoid self-medication without medical advice, especially with regard to medications or exercises that could make the condition worse.
Remember that each case is unique, and recommendations may vary depending on the specific nature of your cervical problems.
Radiographic signs
Commonly looked for radiographic signs include abnormalities in the cervical vertebrae, such as fractures, dislocations or subluxations. Images may show fracture lines, abnormal movement of the vertebrae, or signs of instability. However, soft tissue injuries, which are common in whiplash, are not always clearly visible on standard x-rays.
This is why, in many cases, advanced radiological examinations such as magnetic resonance imaging (MRI) may be recommended. MRI provides a more detailed visualization of soft tissues, including intervertebral discs, ligaments and muscles. It can help identify lesions that might not be detected by conventional x-rays.
Also among the specific radiographic signs looked for are indications of inflammation, edema or hematoma in the cervical region. These elements may indicate an inflammatory response to the injury. Additionally, x-rays may be used to evaluate the overall alignment of the cervical spine and look for structural abnormalities that may be contributing to symptoms.
- Osteoarthritis (Osteoarthritis): Signs of osteoarthritis may appear in the form of degenerative changes in the joints, such as the formation of osteophytes (bone joints) or reduction of joint space.
- Herniated Disc: A herniated disc can be visualized as a displacement or protrusion of the intervertebral disc, possibly putting pressure on adjacent nerve structures.
- Cervical Spondylosis: Cervical spondylosis, characterized by the formation of bony bridges between the vertebrae, can be identified by changes in bone structure.
- Vertebral Instability: Spinal instability, indicating excessive movement between the vertebrae, can be assessed by dynamic radiographs, taken during different neck movements.
- Narrowing of the Spinal Canal: A narrowing of the spinal canal may be observed, which can lead to compression of the spinal cord or nerve roots.
- Spinal Deviations: X-rays can reveal spinal deviations, such as scoliosis, which can influence cervical health.
- Fractures or Dislocations: X-rays can detect possible fractures or dislocations of the vertebrae, often resulting from trauma.
- Joint Erosion: Erosion of joint surfaces may indicate chronic inflammation of the joints.
- Tumors or Masses: The presence of tumors or masses can be detected using x-rays, although other imaging tests may be needed for further evaluation.
It is important to emphasize that the interpretation of cervical x-rays requires medical expertise.

References
- Spitzer WO, et al. Scientific monograph of the Quebec task force on whiplash-associated disorders: redefining “Whiplash” and its management. Spine. 1995;8S:1S–73S. [PubMed] [Google Scholar]
- Cote PDC, Hogg-Johnson S, et al. Initial patterns of clinical care and recovery from whiplash injuries. Arch Intern Med. 2005;165:2257–63. doi: 10.1001/archinte.165.19.2257. [PubMed] [CrossRef] [Google Scholar]
- Cote PDC, Cassidy JDDC, et al. A systematic review of the prognosis of acute whiplash and a new conceptual framework to synthesize the literature. Spine. 2001;26:E445–8. doi: 10.1097/00007632-200110010-00020. [PubMed] [CrossRef] [Google Scholar]
- Eck JC, Hodges SD, Humphreys SC. Whiplash: a review of a commonly misunderstood injury. Am J Med. 2001;110:651–6. doi: 10.1016/S0002-9343(01)00680-5. [PubMed] [CrossRef] [Google Scholar]
- Freeman MD. A review and methodologic critique of the literature refuting whiplash syndrome. Spine. 1999;24:86–98. doi: 10.1097/00007632-199901010-00022. [PubMed] [CrossRef] [Google Scholar]
- Barnsley L, Lord SM, Bogduk N. Pain. 1994;58:283–307. doi: 10.1016/0304-3959(94)90123-6. [PubMed] [CrossRef] [Google Scholar]
- Grauer JN, Panjabi MM, et al. Whiplash produces an S-shaped curvature of the neck with hyperextension at lower levels. Spine. 1997;22:2489–94. doi: 10.1097/00007632-199711010-00005. [PubMed] [CrossRef] [Google Scholar]
- Cassidy JDDC, et al. Effect of eliminating compensation for pain and suffering on the outcome of insurance claims for whiplash injury. N Engl J Med. 2000;342:1179–86. doi: 10.1056/NEJM200004203421606. [PubMed] [CrossRef] [Google Scholar]
- Rodriquez AA, Barr KP, Burns SP. Whiplash: pathophysiology, diagnosis, treatment, and prognosis. Muscle Nerve. 2004;29:768–81. doi: 10.1002/mus.20060. [PubMed] [CrossRef] [Google Scholar]
- Geothem JW, et al. Whiplash injuries: is there a role for imaging? Eur J Radiol. 1996;22:30–37. doi: 10.1016/0720-048X(95)00696-N. [PubMed] [CrossRef] [Google Scholar]
- Ronnen HR, Korte PJ, et al. Acute whiplash injury: is there a role for mr imaging?—a prospective study of 100 patients. Radiology. 1996;201(1):93–6. [PubMed] [Google Scholar]
- Petterson K, et al. Disc pathology after whiplash injury: a prospective magnetic resonance imaging and clinical investigation. Spine. 1997;22:283–7. doi: 10.1097/00007632-199702010-00010. [PubMed] [CrossRef] [Google Scholar]
- Borchegrevnik GE, Kaasa A, McDonagh D, et al. Acute treatment of whiplash neck sprain injuries. Spine 1998;23:25–31. [PubMed]
- Rosenfeld M, Seferiadis A, Carlsson J, Gunnarsson R. Active intervention in patient with whiplash-associated disorder improves long-term prognosis. Spine. 2003;28:2491–8. doi: 10.1097/01.BRS.0000090822.96814.13. [PubMed] [CrossRef] [Google Scholar]
- Petterson K, Toolanen G. High-dose methylprednisolone prevents extensive sick leave after whiplash injury. a prospective, randomised, double-blind study. Spine. 1998;23:984–9. doi: 10.1097/00007632-199805010-00004. [PubMed] [CrossRef] [Google Scholar]
- Vendrig AA, Akkerveeken PF, McWhorter KR. Results of a multimodal treatment program for patients with chronic symptoms after a whiplash injury of the neck. Spine. 2000;25:238–44. doi: 10.1097/00007632-200001150-00016. [PubMed] [CrossRef] [Google Scholar]
- Bunketorp L, Lindh M, Carlsson J, Stene-Victorin E. The perception of pain and pain related cognition in subacute whiplash-associated disorders: its influence on prolonged disability. Disabil Rehabil. 2006;28:271–9. doi: 10.1080/09638280500158323. [PubMed] [CrossRef] [Google Scholar]
- Prushansky T, Pevzner E, Gordon C, Dvir Z. Cervical radiofrequency neurotomy in patients with chronic whiplash: a study of multiple outcome measures. J Neurosurg. 2006;4:365–73. [PubMed] [Google Scholar]





")











{kind=link}