

Morton’s neuroma causes burning pain, tenderness, and paresthesias in the forefoot due to interdigital nerve enlargement from compression, often between the third and fourth toes.
Introduction
Morton’s neuroma is a common yet often overlooked foot condition that can significantly impact an individual’s mobility and quality of life. It is characterized by a thickening of the interdigital nerve, typically occurring between the third and fourth toes. This nerve enlargement results from chronic compression or irritation, leading to symptoms such as sharp, burning pain, tingling, or numbness in the forefoot. Often exacerbated by walking, running, or wearing tight shoes, Morton’s neuroma can transform simple daily activities into painful challenges.
Though the condition is generally benign, its effects are far-reaching, particularly for individuals who lead active lifestyles. Morton’s neuroma is more prevalent in women, likely due to the frequent use of high-heeled or narrow-toed footwear. However, it also affects athletes and others who engage in repetitive, high-impact activities that place excessive stress on the feet. Despite its prevalence, the condition is frequently misdiagnosed or mistaken for other foot problems, delaying proper treatment and prolonging discomfort.
Overview of Morton’s Neuroma
Morton’s neuroma, also referred to as interdigital neuroma or plantar nerve entrapment, was first described in 1876 by Thomas George Morton, a 19th-century Scottish surgeon. It arises when the interdigital nerve becomes trapped or compressed between the metatarsal heads in the forefoot. This leads to irritation, inflammation, and eventual thickening of the nerve, which contributes to the characteristic symptoms.
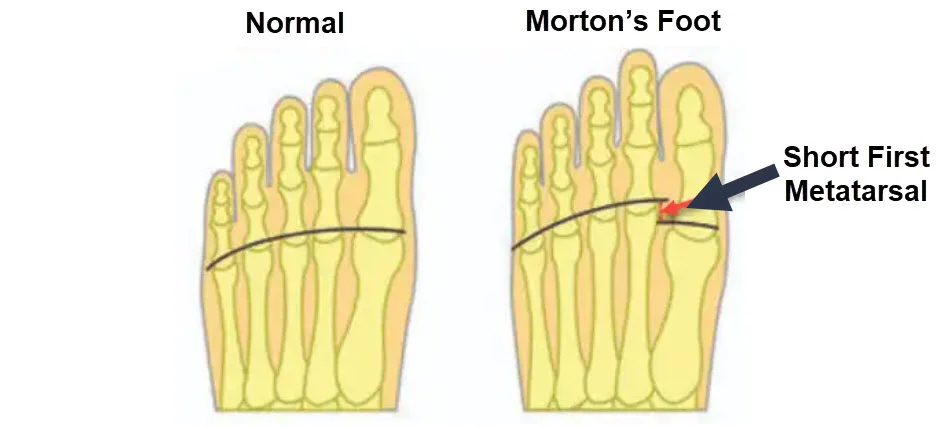
The development of Morton’s neuroma is influenced by various factors, including foot structure, footwear choices, and activity level. Anatomical predispositions such as flat feet, high arches, or structural abnormalities like Morton’s foot (a shortened first metatarsal) can increase the risk. External factors, particularly poorly fitting shoes, play a critical role in exacerbating nerve compression. Additionally, trauma or repetitive stress from activities like running or jumping can aggravate the condition.
Why It Matters: Impact on Quality of Life
Morton’s neuroma can profoundly affect an individual’s quality of life, particularly if left untreated. The condition not only causes physical pain but can also lead to emotional and psychological distress. Persistent discomfort may limit physical activity, reducing opportunities for exercise and social engagement. Over time, this restriction can lead to weight gain, loss of fitness, and even secondary health issues such as joint problems or reduced cardiovascular health.
In professional or athletic contexts, Morton’s neuroma can hinder performance, disrupt training schedules, and necessitate lifestyle changes. For others, the condition might interfere with basic daily tasks like standing for long periods, walking, or wearing formal footwear, further diminishing confidence and independence. Early diagnosis and intervention are essential to managing symptoms and preventing long-term complications, ensuring a better quality of life for those affected.
Anatomy and Biomechanics
Understanding the anatomy and biomechanics of the foot is essential to grasp the development and impact of Morton’s neuroma. The condition arises from the interplay of nerve structures, weight transfer mechanisms, and structural abnormalities, such as Morton’s foot. These factors work together to create the perfect environment for nerve irritation and compression, leading to the characteristic symptoms of pain and discomfort.
Structure of the Interdigital Nerves
The interdigital nerves, also known as plantar digital nerves, are branches of the medial and lateral plantar nerves. These nerves travel between the metatarsal bones and run under the transverse intermetatarsal ligament. They are responsible for providing sensation to the adjacent sides of the toes, playing a vital role in maintaining foot sensitivity and proprioception.
In Morton’s neuroma, the interdigital nerve most commonly affected is located between the third and fourth metatarsals, although the second and third intermetatarsal spaces may also be involved. The nerve becomes compressed due to its anatomical position and the forces exerted on the foot during activities like walking or running. Repeated pressure or irritation causes thickening of the nerve tissue, resulting in pain and other symptoms such as tingling or numbness. The anatomical tightness of the intermetatarsal spaces makes these nerves particularly vulnerable to compression, especially when exacerbated by external factors like tight footwear or high-impact activities.
Weight Transfer Mechanisms in the Foot
The biomechanics of weight transfer in the foot are intricate and essential for efficient movement. During walking or running, the foot absorbs and redistributes forces as it moves through the gait cycle. This process begins with heel strike, progresses through midstance, and ends with toe-off, where the weight is transferred forward to propel the body.
In a healthy foot, the first metatarsal and the big toe play a primary role in bearing weight during the toe-off phase. However, when the normal weight transfer mechanism is disrupted—due to anatomical abnormalities or improper footwear—excessive stress is shifted to other parts of the foot. In the case of Morton’s neuroma, this stress often concentrates on the second, third, and fourth metatarsals, leading to nerve compression and irritation.
Morton’s Foot: A Structural Perspective
Morton’s foot, or the toe is shorter, is often the cause of Morton’s neuroma. Instead of receiving the force of pushing from the foot on the first metatarsal, this load will be transferred laterally, that is to say on the other metatarsals. So, this increased pressure on the other metatarsals would be a reason for the development of Morton’s neuroma.
Lateral weight transfer mechanism with Morton’s foot
When the foot makes contact with the ground, it initiates a complex weight transfer process which plays an essential role in the biomechanics of the foot. This process begins at the heel and then naturally moves toward the first metatarsal, particularly the big toe.

Heel on the Ground: The gait cycle starts with the heel making initial contact with the ground. This phase absorbs the impact of body weight and initiates forward momentum.
Full Ground Contact with the Forefoot: As the gait progresses, the entire forefoot comes into contact with the ground. At this point, the foot acts as a stable platform to distribute body weight evenly, preparing for propulsion.
Heel Lift: The heel rises off the ground as the body weight shifts forward onto the forefoot. The transfer of weight is concentrated on the toes, with the great toe beginning to play a crucial role in stabilization and propulsion.
Toe Off: The gait cycle concludes as the toes, especially the great toe, push the foot off the ground. This phase generates forward propulsion, driving the body into the next step.
A longer great toe improves leverage during the toe-off phase, enhancing stability and efficiency in movement. It allows for better weight transfer, reducing strain on other parts of the foot and ensuring a smooth transition between steps.
The anatomical design of the foot reflects this sequence, as the big toe is designed to effectively receive the load of weight transfer when walking or running.
However, anatomical variations can influence this pattern of weight transfer, leading to adjustments in how the foot absorbs pressure. One of these variations concerns the length of the first metatarsal. If the first metatarsal is shorter than normal (Morton’s foot), the foot must compensate by performing a supination movement. Supination is a movement of the foot that occurs as it rolls outward, directing weight toward the lateral side of the foot.

The image illustrates the biomechanical implications of Morton’s foot, which is a structural variation where the first metatarsal is shorter than the second. This condition alters the normal weight transfer during the gait cycle, leading to potential foot problems and discomfort.
Heel on the Ground: During the initial contact, the heel absorbs the body’s impact force. In Morton’s foot, this phase is unaffected.
Full Ground Contact with the Forefoot: As the forefoot contacts the ground, the shorter first metatarsal shifts weight distribution laterally. Instead of the weight transferring through the medial arch and great toe, it flows toward the second and third metatarsals.
Heel Lift: During this phase, the disproportionate load on the lateral metatarsals increases. The altered biomechanics result in heightened friction and pressure on the interdigital nerves, particularly between the third and fourth toes, where Morton’s neuroma often develops.
Toe Off: The inefficient weight transfer bypasses the great toe, forcing the smaller toes to compensate, leading to overuse and strain.
Morton’s foot is not a normal foot structure. The lateral weight shift caused by the shorter first metatarsal predisposes individuals to forefoot pain, calluses, and nerve irritation (Morton’s neuroma). Custom orthotics and foot-strengthening exercises can help manage these biomechanical challenges.
In this situation, the natural path of weight transfer towards the big toe is modified. Instead, the weight is directed to the second and third metatarsals, which are not necessarily adapted to support such a load. This redistribution of forces can lead to problems, including the formation of corns in the area of the metatarsal heads of the second and third metatarsals.
Morton’s neuroma, a painful condition, is often seen in this setting, particularly between the third and fourth metatarsal heads. Morton’s neuroma is a condition resulting from compression of the interdigital plantar nerve, usually between these two metatarsals. This compression can be accentuated by the change in the weight transfer pattern caused by supination of the foot.
Symptoms of Morton’s neuroma include shooting pain, tingling, or burning sensation between the toes, usually between the third and fourth toes. These symptoms may worsen while walking, running, or wearing tight shoes. The specific location of the symptoms is linked to the compression of the nerve in the region of the metatarsal heads, accentuated by the supination of the foot due to the reduced length of the first metatarsal
Causes and Risk Factors
Morton’s neuroma, a condition characterized by thickening of the interdigital nerve due to irritation or compression, is influenced by a variety of intrinsic and extrinsic factors. Understanding the causes and risk factors is essential for identifying individuals at risk and implementing preventative measures. The development of this painful condition often involves a combination of anatomical predispositions, biomechanical abnormalities, lifestyle choices, and external influences such as footwear.
Common Triggers of Morton’s Neuroma
At the root of Morton’s neuroma lies the compression or irritation of the interdigital nerve, most often in the third intermetatarsal space. Common triggers include repeated stress or trauma to the forefoot, which can lead to inflammation and nerve thickening. Activities that involve repetitive impact, such as running or jumping, are particularly problematic. Furthermore, conditions such as bunions, hammertoes, or flat feet may predispose individuals to altered foot mechanics, increasing the likelihood of nerve entrapment.
Age and sex also play a role. The condition is more prevalent in middle-aged women, which may be due to lifestyle factors, including footwear choices. Additionally, anatomical variations like a short first metatarsal, known as Morton’s foot, can exacerbate the redistribution of forces across the forefoot, further contributing to nerve compression.
Biomechanical Abnormalities (e.g., Supination, Pronation)
Biomechanical abnormalities significantly influence the development of Morton’s neuroma. Both supination and pronation can alter the natural weight transfer in the foot, increasing stress on specific areas.
Supination, a condition where the foot rolls outward during movement, shifts weight laterally, placing excessive pressure on the metatarsal heads. This lateral weight transfer can lead to nerve compression between the metatarsal bones, particularly in individuals with anatomical predispositions like Morton’s foot.
Conversely, pronation, where the foot rolls inward excessively, can also contribute to nerve irritation. In cases of overpronation, the natural alignment of the metatarsals is disrupted, causing uneven weight distribution. This creates additional stress on the intermetatarsal spaces and the nerves passing through them. Over time, these biomechanical abnormalities can result in chronic irritation, inflammation, and eventual nerve thickening, leading to Morton’s neuroma.
Role of Footwear: High Heels and Tight Shoes
Footwear is one of the most significant external factors contributing to Morton’s neuroma. Shoes that are too tight or have pointed toes can compress the forefoot, restricting the natural spread of the toes and placing additional pressure on the interdigital nerves. High-heeled shoes exacerbate the issue by shifting the body’s weight forward, concentrating pressure on the ball of the foot and the metatarsal heads.
Women, who are more likely to wear high heels or narrow-toed shoes, are disproportionately affected by Morton’s neuroma. This is compounded by the repetitive stress placed on the feet, as tight and poorly fitting footwear limits the foot’s ability to function properly and absorb shock. The combination of compression and high-pressure zones in the forefoot makes these shoes a significant risk factor.
Lifestyle and Activities: High-Impact Sports
Active lifestyles, particularly those involving high-impact sports, increase the risk of Morton’s neuroma. Activities such as running, basketball, or tennis generate repeated forceful impacts on the forefoot. Over time, this constant pressure can lead to inflammation, nerve irritation, and eventual neuroma formation.
Sports that involve sudden stops and starts or lateral movements can further strain the intermetatarsal spaces, increasing the likelihood of nerve compression. Athletes who already have biomechanical abnormalities or wear ill-fitting sports shoes are particularly vulnerable.
Symptoms and Clinical Presentation
Morton’s neuroma, a condition involving the thickening of the interdigital nerve, manifests with a range of symptoms primarily localized to the forefoot. These symptoms, while often straightforward in presentation, can significantly affect daily activities, making it essential to understand the pain patterns and associated sensations that characterize the condition.
Pain Patterns and Characteristics
Pain is the most defining symptom of Morton’s neuroma. It is typically localized to the ball of the foot, often between the third and fourth toes, though the second and third interdigital spaces can also be affected. The pain is usually described as burning, stabbing, or sharp and may radiate toward the toes. Many patients liken the sensation to stepping on a pebble or having a small object lodged in their shoe, which often prompts them to check their footwear.
This pain pattern is activity-dependent in the early stages of the condition. Weight-bearing activities, such as walking, running, or prolonged standing, can exacerbate the discomfort, as can wearing tight, high-heeled, or narrow-toed shoes that compress the forefoot. Conversely, removing footwear, massaging the affected area, or resting the foot often provides temporary relief.
The pain may also radiate along the distribution of the interdigital nerve, extending to the adjacent sides of the affected toes. This radiating characteristic is a diagnostic hallmark that distinguishes Morton’s neuroma from other causes of forefoot pain, such as metatarsalgia, where the pain is more diffuse and less localized to a nerve distribution.
As the condition progresses, the pain may become more frequent and intense, sometimes persisting even at rest. Advanced cases can lead to chronic discomfort, significantly impairing mobility and quality of life.
Numbness and Tingling Sensations
In addition to pain, Morton’s neuroma is often associated with sensory disturbances, such as numbness and tingling in the toes. These sensations occur because the interdigital nerve, which transmits sensory signals to the adjacent sides of the toes, becomes compressed or irritated. This disruption in nerve function results in paresthesias that range from mild tingling to a persistent pins-and-needles sensation.
The numbness often affects the sides of the toes adjacent to the affected nerve. Patients may notice decreased sensitivity in these areas, which can interfere with proprioception and foot mechanics. This loss of sensation may be intermittent initially, triggered by specific activities like walking or wearing tight shoes. Over time, as the condition worsens, numbness may become constant and more pronounced.
Tingling sensations, similar to electrical shocks, may intensify during activities that compress the nerve, such as standing for prolonged periods or engaging in high-impact sports. Patients often describe these sensations as annoying or unsettling, as they can occur unpredictably and disrupt normal activities.
These sensory disturbances, particularly when combined with localized pain, are key features that point to Morton’s neuroma. While other conditions, such as tarsal tunnel syndrome or diabetic neuropathy, can also cause numbness and tingling, these symptoms are typically more diffuse and not confined to the interdigital spaces.
Diagnosis
Accurate diagnosis of Morton’s neuroma is critical to effectively manage and treat the condition. A thorough evaluation, including a detailed clinical examination, imaging studies, and consideration of other potential causes, helps ensure that the symptoms are correctly attributed to Morton’s neuroma. The diagnostic process focuses on identifying the hallmark features of the condition, ruling out other potential diagnoses, and determining the severity of nerve involvement.
Clinical Examination and Key Signs
The diagnostic journey typically begins with a clinical examination and detailed patient history. Key symptoms such as burning pain, tingling, numbness, or the sensation of a pebble in the shoe often lead patients to seek medical advice. The pain is usually localized in the forefoot, commonly between the third and fourth toes, and may worsen with walking, running, or wearing tight shoes. Symptoms often improve with rest or removal of restrictive footwear.
During the physical examination, specific maneuvers are performed to elicit pain and confirm the presence of Morton’s neuroma. A common technique is the Mulder’s Sign, which involves squeezing the metatarsal heads together while applying pressure to the affected intermetatarsal space. A palpable “click” or reproduction of symptoms during this test strongly suggests nerve compression. Additionally, palpation may reveal tenderness or a thickened area in the affected region, further supporting the diagnosis.
While clinical examination provides valuable insights, its accuracy can be influenced by factors such as overlapping symptoms with other conditions. For this reason, imaging techniques are often employed to confirm the diagnosis.
Imaging Techniques: X-rays, Ultrasound, and MRI
X-rays are typically the first imaging modality used, primarily to exclude other conditions such as fractures, arthritis, or structural abnormalities that could mimic Morton’s neuroma. Although X-rays cannot directly visualize the neuroma, they help rule out alternative causes of forefoot pain.
Ultrasound is a widely used tool for diagnosing Morton’s neuroma due to its ability to visualize soft tissues and provide real-time imaging. It can accurately identify thickened interdigital nerves, usually appearing as hypoechoic (dark) masses between the metatarsal heads. Ultrasound is non-invasive, cost-effective, and allows for dynamic assessment, making it a preferred choice in many clinical settings.
Magnetic Resonance Imaging (MRI) offers the highest sensitivity and specificity for diagnosing Morton’s neuroma. MRI can detect nerve thickening and assess surrounding structures with detailed resolution. This modality is particularly useful in complex cases where the diagnosis is unclear or when surgical intervention is being considered. MRI also helps rule out other soft-tissue conditions such as tumors or tendon injuries that may mimic Morton’s neuroma.
Differential Diagnosis
A thorough differential diagnosis is essential to distinguish Morton’s neuroma from other conditions that cause similar symptoms. Common conditions that mimic Morton’s neuroma include:
- Metatarsalgia: Generalized pain in the ball of the foot caused by inflammation or overuse, often without nerve involvement.
- Stress Fractures: Fractures of the metatarsal bones can cause localized pain similar to Morton’s neuroma but are typically identified on X-rays or MRI.
- Capsulitis or Synovitis: Inflammation of the joint capsules or synovial tissues around the metatarsals may mimic the localized pain of a neuroma.
- Tarsal Tunnel Syndrome: Nerve entrapment in the ankle region can cause referred pain to the forefoot but involves different nerve pathways.
- Plantar Plate Tears: Damage to the ligamentous structures supporting the metatarsophalangeal joint can lead to forefoot pain and instability, often mistaken for Morton’s neuroma.
- Neuropathies: Conditions such as diabetic neuropathy or peripheral neuropathy can produce tingling or burning sensations in the feet, requiring careful evaluation to differentiate from Morton’s neuroma.
Historical Context
Thomas George Morton: Pioneer of Morton’s Neuroma Research
Thomas George Morton (1835–1903), a 19th-century Scottish-American surgeon and anatomist, was the first to describe what is now known as Morton’s neuroma. His pioneering work laid the foundation for understanding this painful foot condition, characterized by thickening of the interdigital nerve due to compression or irritation between the metatarsal heads. Morton’s first formal description of the condition appeared in 1876, where he emphasized the role of nerve entrapment and localized pressure in the forefoot as critical factors in symptom development.
1835–1903
Morton’s observations were groundbreaking for his time, highlighting the importance of anatomical variations and external influences, such as footwear, in exacerbating nerve compression. His meticulous documentation of symptoms like burning pain, numbness, and a foreign-body sensation between the toes became the cornerstone for identifying Morton’s neuroma in clinical practice. The condition was later named in his honor, cementing his legacy in the field of orthopedic and neurological foot disorders.
Although the condition itself likely existed long before Morton’s description, his contributions were instrumental in advancing medical understanding and inspiring further research. Morton’s work demonstrated the importance of considering biomechanical and structural factors in diagnosing and treating foot pain, paving the way for modern approaches to patient care.
Evolution of Diagnostic and Treatment Approaches
Since Morton’s initial description, the understanding of Morton’s neuroma has evolved significantly, driven by advances in medical imaging, surgical techniques, and biomechanics. Early diagnostic approaches relied heavily on clinical examination and patient-reported symptoms, as imaging technologies like X-rays were not yet widely available. While these methods were valuable, they were limited in their ability to confirm the presence of nerve thickening or rule out other conditions with similar symptoms.
The advent of modern imaging modalities, such as ultrasound and magnetic resonance imaging (MRI), revolutionized the diagnostic process by enabling direct visualization of the interdigital nerve and surrounding structures. These technologies provide high-resolution images that allow clinicians to detect nerve enlargement, inflammation, and other abnormalities with greater accuracy. Ultrasound, in particular, has become a preferred diagnostic tool due to its non-invasive nature, real-time assessment capabilities, and cost-effectiveness.
Treatment approaches have also progressed significantly. Initially, management focused on symptomatic relief through conservative measures like rest, changes in footwear, and physical therapy. Over time, more advanced interventions were developed, including corticosteroid injections, alcohol ablation, and, in severe cases, surgical excision of the neuroma. These advancements have expanded treatment options, allowing for more personalized care based on the severity of symptoms and patient preferences.
Today, Morton’s neuroma is recognized as a condition influenced by a combination of anatomical, biomechanical, and lifestyle factors. This multidimensional understanding, coupled with ongoing research, continues to improve diagnostic accuracy and therapeutic outcomes, ensuring that Morton’s legacy as a pioneer in medical science endures.
Summary
The interdigital nerves navigate through the space between the metatarsal heads, close to the bottom of the foot, passing under the ligaments that join the adjacent metatarsal heads. These nerves are responsible for carrying sensation to the medial and lateral sides of the adjacent toes.
Morton’s neuroma represents an alteration of these nerves in the anterior region of the foot. The most common symptom is pain felt directly between the metatarsal heads. Typically, only one nerve is affected, although cases involving multiple nerves can occur. The most common location of an interdigital neuroma is between the third and fourth toes, but it is not uncommon to see neuromas between the second and third toes.

Osteopathy and the Conservative Approach to Morton’s Neuroma
Osteopathy offers a holistic and patient-centered approach to managing Morton’s neuroma, focusing on alleviating symptoms, improving foot mechanics, and addressing underlying causes without invasive interventions. By emphasizing the body’s natural ability to heal itself, osteopathic treatment aims to restore balance and function, reduce pain, and prevent the progression of the condition.
Principles of Osteopathic Care
Osteopathy operates on several foundational principles that guide the treatment of Morton’s neuroma:
- The Body is a Unit: The foot does not function in isolation but as part of a complex biomechanical chain involving the entire body. Addressing alignment and movement patterns in the lower extremity, pelvis, and spine is essential for effective treatment.
- Self-Healing and Regulation: The body has an inherent ability to repair itself. Osteopathic treatment supports this process by improving circulation, reducing nerve compression, and promoting tissue health.
- Structure and Function are Interrelated: Alterations in foot structure, such as pronation, supination, or a shortened first metatarsal (Morton’s foot), can disrupt function and lead to nerve compression. Correcting these dysfunctions is a key focus of osteopathic care.
Techniques in Osteopathy for Morton’s Neuroma
Osteopathic treatment for Morton’s neuroma employs a variety of techniques tailored to the individual’s needs and the severity of their condition. These techniques aim to reduce pain, restore mobility, and improve foot mechanics:
- Soft Tissue Techniques
Soft tissue manipulation is used to reduce tension in the muscles, tendons, and fascia of the foot and lower leg. By relieving tightness in the plantar fascia, calf muscles, and intrinsic foot muscles, osteopaths can decrease pressure on the metatarsals and interdigital nerves. This improves local circulation and reduces inflammation, promoting natural healing. - Myofascial Release
This technique targets the fascia—the connective tissue surrounding muscles and nerves. By releasing fascial restrictions in the foot and lower leg, osteopaths help to alleviate nerve compression and improve the foot’s ability to adapt to weight-bearing activities. - Articulatory Techniques
Gentle mobilization of the foot joints can improve the alignment of the metatarsals and reduce mechanical stress on the interdigital nerves. These techniques are particularly useful in restoring the natural weight transfer mechanism of the foot. - Cranial and Sacral Adjustments
The foot’s function is closely connected to the pelvis and spine. By addressing imbalances in these areas, osteopaths can improve overall posture and gait mechanics, reducing stress on the foot. - Visceral Manipulation
In some cases, visceral techniques may be used to address systemic factors, such as poor circulation or inflammation, that may contribute to foot pain.
Lifestyle and Functional Advice
In addition to hands-on techniques, osteopaths provide guidance on lifestyle modifications and functional strategies to prevent recurrence and support recovery:
- Footwear Recommendations
Osteopaths often advise wearing shoes with a wide toe box, adequate arch support, and cushioning to reduce pressure on the forefoot. High heels and narrow-toed shoes should be avoided. - Orthotic Support
Custom orthotic insoles may be recommended to correct biomechanical abnormalities, such as overpronation or uneven weight distribution, that contribute to nerve compression. - Exercise Prescription
Strengthening and stretching exercises for the foot and lower leg muscles are often incorporated into treatment plans. These exercises improve flexibility, support the foot’s arch, and enhance overall foot function. - Activity Modifications
High-impact activities, such as running, may need to be temporarily reduced or adjusted to minimize stress on the forefoot. Osteopaths guide patients on how to transition to lower-impact alternatives and gradually return to regular activities.
Conclusion
In conclusion, Morton’s neuroma represents a challenge for those who suffer from it, significantly impacting their daily lives. A thorough understanding of this condition, its underlying causes and possible interventions is essential for effective management. Whether through conservative approaches such as wearing appropriate shoes, using orthotics, or more advanced options like corticosteroid injections or, in severe cases, surgery, treatment for Morton’s neuroma can be adapted according to the severity of the symptoms. It is recommended to consult a healthcare professional for an accurate diagnosis and personalized treatment plan, allowing individuals to regain optimal quality of life while minimizing the effects of this painful condition.
References
- Ruiz Santiago F, Prados Olleta N, Tomás Muñoz P, Guzmán Álvarez L, Martínez Martínez A. Short term comparison between blind and ultrasound guided injection in morton neuroma. Eur Radiol. 2019 Feb;29(2):620-627. [ PubMed ]
- Ganguly A, Warner J, Aniq H. Central Metatarsalgia and Walking on Pebbles: Beyond Morton Neuroma. AJR Am J Roentgenol. 2018 Apr;210(4):821-833. [ PubMed ]
- Lorenzon P, Rettore C. Mechanical Metatarsalgia as a Risk Factor for Relapse of Morton’s Neuroma After Ultrasound-Guided Alcohol Injection. J Foot Ankle Surg. 2018 Sep – Oct;57(5):870-875. [ PubMed ]
- Di Caprio F, Meringolo R, Shehab Eddine M, Ponziani L. Morton’s interdigital neuroma of the foot: A literature review. Foot Ankle Surg. 2018 Apr;24(2):92-98. [ PubMed ]
- Edenfield KM, Michaudet C, Nicolette GW, Carek PJ. Foot and Ankle Conditions: Midfoot and Forefoot Conditions. FP Essent. 2018 Feb;465:30-34. [ PubMed ]
- Santiago FR, Muñoz PT, Pryest P, Martínez AM, Olleta NP. Role of imaging methods in diagnosis and treatment of Morton’s neuroma. World J Radiol. 2018 Sep 28;10(9):91-99. [ PMC free article ] [ PubMed ]
- LiMarzi GM, Scherer KF, Richardson ML, Warden DR, Wasyliw CW, Porrino JA, Pettis CR, Lewis G, Mason CC, Bancroft LW. CT and MR Imaging of the Postoperative Ankle and Foot. Radiographics. 2016 Oct;36(6):1828-1848. [ PubMed ]
- Naraghi R, Bremner A, Slack-Smith L, Bryant A. The relationship between foot posture index, ankle equinus, body mass index and intermetatarsal neuroma. J Foot Ankle Res. 2016;9:46. [ PMC free article ] [ PubMed ]
- Naraghi R, Bremner A, Slack-Smith L, Bryant A. Radiographic Analysis of Feet With and Without Morton’s Neuroma. Foot Ankle Int. 2017 Mar;38(3):310-317. [ PubMed ]
- Masala S, Cuzzolino A, Morini M, Raguso M, Fiori R. Ultrasound-Guided Percutaneous Radiofrequency for the Treatment of Morton’s Neuroma. Cardiovasc Intervent Radiol. 2018 Jan;41(1):137-144. [ PubMed ]
- Lizano-Díez : A Prospective, Double-Blinded, Randomized, Placebo-Controlled Trial. Foot Ankle Int. 2017 Sep;38(9):944-951. [ PubMed ]
- Lee J, Kim J, Lee M, Chu I, Lee S, Gwak H. Morton’s Neuroma (Interdigital Neuralgia) Treated with Metatarsal Sliding Osteotomy. Indian J Orthop. 2017 Nov-Dec;51(6):692-696. [ PMC free article ] [ PubMed ]
- Credit in part: Usama Munir; Dawood Tafti; Samer Morgan.


















{kind=link}