

Understanding Genitofemoral Neuralgia: A Little-Known Nerve, A Real Pain
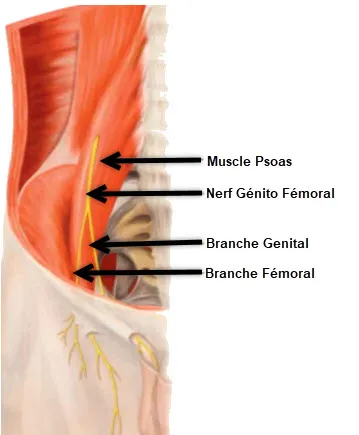
Genitofemoral neuralgia is a medical condition characterized by pain along the path of the genitofemoral nerve. This nerve, originating from the L1 and L2 nerve roots of the spinal cord, innervating the genital region and the anterior aspect of the thigh, can be subject to irritation or compression, resulting in the manifestation of painful symptoms.
Symptoms of genitofemoral neuralgia are often described as sharp, burning, tingling, or electric shock-like sensations along the nerve’s path. The pain can radiate from the genital area to the front of the thigh, causing significant discomfort for affected individuals.
The causes of genitofemoral neuralgia can be varied. Nerve compression can result from anatomical disorders such as inguinal hernias, trauma, or even surgical procedures in the pelvic region. Inflammatory or infectious conditions can also contribute to the development of this neuralgia.
The impact of genitofemoral neuralgia on patients’ quality of life is often underestimated. Severe pain can interfere with daily activities, personal relationships, and even sleep. Due to the specific location of the genitofemoral nerve, the condition can also pose unique emotional and psychological challenges.
Diagnosis of genitofemoral neuralgia is based on clinical assessment of symptoms, possibly supplemented by medical imaging tests such as MRIs or CT scans to identify the source of nerve irritation. It is crucial to rule out other possible causes of pelvic pain before confirming the diagnosis.
Management of genitofemoral neuralgia may involve a multidisciplinary approach. Treatment options may include analgesic medications to relieve pain, osteopathic interventions to improve mobility and reduce nerve compression, and more invasive approaches such as nerve blocks or electrical stimulation.
It is essential to adopt a holistic approach to managing genitofemoral neuralgia. Pain management, physical rehabilitation, and psychological support can play a crucial role in improving the quality of life of those affected. Regular follow-up with healthcare professionals allows the treatment plan to be adjusted based on the patient’s individual response.
Genitofemoral neuralgia is a condition that can significantly impact the daily lives of those who suffer from it. Understanding the symptoms, possible causes, and available treatment options is essential to providing effective support to individuals affected by this neuralgia. An integrated approach, involving different medical disciplines, can help alleviate pain and improve patients’ overall quality of life.
Typical Symptoms: When Pain Follows the Nerve
Symptoms of genitofemoral neuralgia can vary from person to person, but are usually related to irritation or compression of the genitofemoral nerve. Common manifestations of this condition include:
- Pain along the nerve: Pain is the main symptom of genitofemoral neuralgia. It can manifest as sharp pain, burning, tingling, or electric shock sensations along the path of the genitofemoral nerve.
- Radiation to the genital area and thigh: Pain may radiate from the genital area to the front of the thigh. This creates a widespread area of tenderness along the affected nerve.
- Pelvic area discomfort: Patients may experience discomfort in the pelvic area, and this sensation may be exacerbated by certain body movements or positions.
- Increased sensitivity: Increased sensitivity may be present along the course of the genitofemoral nerve. Tight clothing or physical contact may aggravate the pain.
- Impaired quality of life: Due to the specific location of the genitofemoral nerve, neuralgia can impact daily life, including physical activities, intimate relationships, and even sleep.
- Numbness: Some individuals with genitofemoral neuralgia may experience numbness along the nerve’s path, in addition to pain and tingling sensations.
- Muscle weakness: Prolonged compression of the genitofemoral nerve can lead to muscle weakness in the thigh or pelvic region.
- Sensitivity disturbances: Alterations in sensitivity, such as decreased tactile sensation or changes in temperature perception, may also be observed.
- Autonomic reactions: Some patients may experience autonomic reactions, such as changes in sweating or changes in skin color in the affected area.
- Worsening with certain movements: Symptoms of genitofemoral neuralgia may worsen with certain specific body movements, physical activities, or even prolonged sitting.
- Impact on sexual quality of life: Due to the innervation of the genital region by the genitofemoral nerve, this condition can also influence the sexual quality of life of affected individuals.
Pain in Women, Pain in Men: Variations by Sex
Genitofemoral neuralgia, although it can affect both sexes, can present differently in men and women. Symptoms reported by men suffering from this condition frequently include localized pain in the groin and testicles, creating a deep and often persistent feeling of pain.
For men, pain in the groin area can be particularly debilitating, affecting not only their daily physical comfort but also their daily activities and overall well-being. The pain can manifest as burning, tingling, or even a dull, constant ache.
On the other hand, in women with genitofemoral neuralgia, symptoms are often reported in specific areas of the genital tract. Pain is most commonly felt in the clitoris and labia majora. This specific location of pain can lead to additional difficulties, particularly regarding sexuality and general physical comfort.
When genitofemoral neuralgia affects the clitoris and labia majora in women, it can directly influence sensory response during sexual activity, leading to complications in the intimate sphere. The pain can also interfere with women’s emotional and psychological well-being, adding a complex dimension to managing this condition.
These differences in symptom location between men and women highlight the complexity of genitofemoral neuralgia and the importance of an individualized approach to diagnosing and managing this condition. Healthcare professionals must take these variations into account to provide personalized treatment tailored to each patient’s specific physiology.
In addition to differences in symptom location, the severity of genitofemoral neuralgia can also vary considerably from person to person. Some individuals may experience intermittent, manageable pain, while others may experience persistent, debilitating pain requiring more intensive medical management.
Recognizing these gender differences in presentation highlights the importance of open communication between patients and healthcare professionals. This allows not only for accurate symptom assessment, but also for treatment planning tailored to the individual needs of each person affected by genitofemoral neuralgia.
Causes of Genitofemoral Neuralgia: What Causes the Pain
The causes of genitofemoral neuralgia are usually related to irritation or compression of the genitofemoral nerve. Several factors can contribute to the development of this condition, including:
- Inguinal hernias: An inguinal hernia, which occurs when part of the abdominal contents pushes through a weak point in the muscular wall of the groin, can put pressure on the genitofemoral nerve, causing irritation.
- Trauma: Direct trauma, such as injuries or accidents, can damage the genitofemoral nerve and lead to inflammation or compression.
- Pelvic surgery: Surgical procedures in the pelvic region, especially those involving the inguinal canal, can cause irritation of the genitofemoral nerve.
- Infections: Infections, such as post-surgical infections or pelvic infections, can contribute to inflammation of the genitofemoral nerve.
- Muscle compression: Certain muscles in the pelvic region can put excessive pressure on the genitofemoral nerve due to muscle spasms or excessive tension.
- Anatomical abnormalities: Congenital or acquired anatomical abnormalities, such as variations in nerve path or spinal abnormalities, may increase the risk of genitofemoral neuralgia.
- Tumors: Although rarer, the presence of tumors in the pelvic region can put pressure on the genitofemoral nerve, causing symptoms.
- Compression during pregnancy: In pregnant women, the growing uterus can sometimes put pressure on the genitofemoral nerve, causing temporary symptoms.
What Pain Hides: Mechanisms and Pathophysiology
The pathophysiology of genitofemoral neuralgia primarily involves irritation or compression of the genitofemoral nerve, a mixed nerve originating from the L1 and L2 nerve roots of the spinal cord. This nerve innervates the genital region and the anterior aspect of the thigh. When subjected to excessive pressure, inflammation, or trauma, it can cause characteristic painful symptoms.
Here are the general stages of the pathophysiology of genitofemoral neuralgia:
- Nerve irritation or compression: Genitofemoral neuralgia often results from irritation or compression of the genitofemoral nerve. This compression can be due to several factors, such as inguinal hernias, trauma, surgery, infections, or other medical conditions.
- Local inflammation: Irritation of the genitofemoral nerve can trigger a local inflammatory response. Inflammation contributes to the release of pro-inflammatory chemicals, which worsens painful symptoms.
- Altered nerve conduction: Nerve irritation can alter normal nerve conduction. This can lead to increased nerve sensitivity, causing abnormal sensations such as pain, tingling, and numbness.
- Central nervous system response: Pain signals from the genitofemoral nerve can be interpreted and amplified by the central nervous system. This contributes to pain perception and can result in an amplified response to normal stimuli.
- Adaptive responses: In response to pain, the body may develop adaptive responses, such as changes in posture or alterations in gait pattern. These adjustments can, in turn, lead to musculoskeletal imbalances and worsen symptoms.
It is important to note that genitofemoral neuralgia can have variable manifestations from person to person depending on the underlying cause, the severity of nerve irritation, and other individual factors. In addition, the specific pathophysiology may vary depending on the initial cause of nerve irritation.
Making an Accurate Diagnosis: Identifying Neuralgia with Clarity
Diagnosis of genitofemoral neuralgia requires a methodical approach, as this condition can mimic other pelvic or neurological pain. Due to its relative rarity and the complexity of the anatomical region involved, it is sometimes underdiagnosed or confused with other pathologies such as inguinal hernia, ilioinguinal neuralgia, or pain of urological or gynecological origin. A rigorous clinical evaluation is therefore essential to make a reliable diagnosis.
Listening attentively to the patient: the first key
The starting point is always the anamnesis, that is, listening carefully to the patient’s complaints. The clinician should look for pain localized in the inguinal, genital, or anterior thigh region , often described as burning, tingling, or electric shocks. The patient may also report hypersensitivity to touch , discomfort when sitting for long periods , or difficulties in the sexual sphere .
Particular attention is paid to the circumstances in which the symptoms appeared : recent surgery (herniorrhaphy, cesarean section), pregnancy, trauma, or simply spontaneous development. The intensity and functional impact on daily life (sleep, intimacy, work) should also be explored.
Clinical examination: precision and finesse
The physical examination seeks to reproduce symptoms or locate an area of tension. The key test is to palpate the exit point of the genitofemoral nerve , which is located near the anterior superior iliac spine, just above the inguinal ligament. Pressure at this location may cause sharp, radiating pain, confirming nerve involvement.
The clinician can also assess skin sensitivity in the area of nerve innervation (pubis, labia majora or testicles, anterior aspect of the thigh). Asymmetry or hypersensitivity to light pressure may indicate nerve damage.
Other tests are used to eliminate differential diagnoses:
- The Tinel test , applied at the level of the inguinal canal;
- Palpation of the psoas muscle to exclude muscle pain;
- Examination of the lumbar roots L1-L2 to ensure that it is not radiculopathy.
Imaging tests: useful but not systematic support
Imaging is not routinely necessary to diagnose genitofemoral neuralgia, but it can be helpful in cases of diagnostic uncertainty or to rule out other pathologies. Pelvic or abdominopelvic MRI can visualize a hernia, mass, or localized inflammation that may be irritating the nerve. CT scans are sometimes prescribed to explore bone structures or anatomical abnormalities.
MRI neurography , which is rarer, can in certain cases visualize peripheral nerves in high resolution, but is still little used in current practice.
Diagnostic infiltration: a confirmation tool
In case of persistent doubt, targeted anesthetic infiltration of the genitofemoral nerve can be performed under ultrasound guidance. If the infiltration temporarily relieves pain, this constitutes a strong criterion for diagnostic confirmation.
This approach is particularly useful in chronic cases, or when invasive treatment is considered (radiofrequency, neurolysis, etc.).
The role of the osteopath in identification
The osteopath, often consulted for unexplained pelvic pain, can play a valuable role in diagnostic guidance . Through fine palpation, a global assessment of posture, visceral mobility and fascial tension, he can suspect involvement of the genitofemoral nerve and refer the patient for further medical diagnosis if necessary.
Diagnosis: Identifying Genitofemoral Neuralgia Accurately
Diagnosis of genitofemoral neuralgia requires a methodical approach, as this condition can mimic other pelvic or neurological pain. Due to its relative rarity and the complexity of the anatomical region involved, it is sometimes underdiagnosed or confused with other pathologies such as inguinal hernia, ilioinguinal neuralgia, or pain of urological or gynecological origin. A rigorous clinical evaluation is therefore essential to make a reliable diagnosis.
Listening attentively to the patient: the first key
The starting point is always the anamnesis, that is, listening carefully to the patient’s complaints. The clinician should look for pain localized in the inguinal, genital, or anterior thigh region , often described as burning, tingling, or electric shocks. The patient may also report hypersensitivity to touch , discomfort when sitting for long periods , or difficulties in the sexual sphere .
Particular attention is paid to the circumstances in which the symptoms appeared : recent surgery (herniorrhaphy, cesarean section), pregnancy, trauma, or simply spontaneous development. The intensity and functional impact on daily life (sleep, intimacy, work) should also be explored.
The physical examination seeks to reproduce symptoms or locate an area of tension. The key test is to palpate the exit point of the genitofemoral nerve , which is located near the anterior superior iliac spine, just above the inguinal ligament. Pressure at this location may cause sharp, radiating pain, confirming nerve involvement.
The clinician can also assess skin sensitivity in the area of nerve innervation (pubis, labia majora or testicles, anterior aspect of the thigh). Asymmetry or hypersensitivity to light pressure may indicate nerve damage.
Other tests are used to eliminate differential diagnoses:
- The Tinel test , applied at the level of the inguinal canal;
- Palpation of the psoas muscle to exclude muscle pain;
- Examination of the lumbar roots L1-L2 to ensure that it is not radiculopathy.
Imaging tests: useful but not systematic support
Imaging is not routinely necessary to diagnose genitofemoral neuralgia, but it can be helpful in cases of diagnostic uncertainty or to rule out other pathologies. Pelvic or abdominopelvic MRI can visualize a hernia, mass, or localized inflammation that may be irritating the nerve. CT scans are sometimes prescribed to explore bone structures or anatomical abnormalities.
MRI neurography , which is rarer, can in certain cases visualize peripheral nerves in high resolution, but is still little used in current practice.
Diagnostic infiltration: a confirmation tool
In case of persistent doubt, targeted anesthetic infiltration of the genitofemoral nerve can be performed under ultrasound guidance. If the infiltration temporarily relieves pain, this constitutes a strong criterion for diagnostic confirmation.
This approach is particularly useful in chronic cases, or when invasive treatment is considered (radiofrequency, neurolysis, etc.).
The role of the osteopath in identification
The osteopath, often consulted for unexplained pelvic pain, can play a valuable role in diagnostic guidance . Through fine palpation, a global assessment of posture, visceral mobility and fascial tension, he can suspect involvement of the genitofemoral nerve and refer the patient for further medical diagnosis if necessary.
Prevention Tips: Take Action Every Day to Avoid Recurrences
Genitofemoral neuralgia, due to its delicate location and functional impact, requires management that goes beyond the acute treatment phase. Once the pain has been alleviated, it is essential to adopt preventive measures to avoid recurrences, support nerve recovery, and improve quality of life. The osteopath plays a central role in this support phase, providing individualized advice tailored to each patient’s lifestyle.
Improve your posture every day
Posture is one of the fundamental levers in preventing mechanical tension on the genitofemoral nerve. Poor sitting posture, lumbar hyperlordosis, or an unbalanced pelvis can maintain chronic pressure on pelvic structures.
Tips to integrate:
- Use an ergonomic chair with good lumbar support, especially when working in a seated position for long periods.
- Change position regularly , ideally every 30 to 45 minutes.
- Avoid crossing your legs, which can accentuate pelvic twists.
- Place a cushion under your knees when lying down to relieve lower back pain.
The osteopath can guide the patient in analyzing their posture at work and suggest simple but effective adjustments.
Incorporate gentle, regular exercise
Proper physical activity helps improve circulation, reduce muscle tension , and maintain good muscle tone without aggravating symptoms. The goal is to maintain flexibility and muscle balance around the pelvis.
Recommended exercises:
- Gentle stretches of the psoas , adductors and quadriceps muscles ;
- Pelvic mobility movements in the lying position (pelvic tilts, diaphragmatic breathing);
- Slow walking or swimming, without sudden movements.
The key is gradualness : avoid high-impact sports (running, excessive weight training) until the pain is completely under control.
Ergonomics and everyday gestures
Simple habits can limit stress on the pelvic region:
- Use a footrest to relieve lower back strain;
- Avoid clothing that is too tight around the waist or groin;
- Prefer soft , non-compressive underwear ;
- Pay attention to the load-bearing efforts : bend at the knees, avoid sudden twists of the trunk.
A preventive osteopathic assessment allows us to detect emerging tensions before they reactivate pain.
Managing stress and internal tension
Stress is a well-known amplifier of chronic pain. It can increase muscle tone , particularly in the abdominal, pelvic, and diaphragmatic areas, and exacerbate nerve sensitivity.
Recommended strategies:
- Deep breathing techniques (cardiac coherence, abdominal breathing);
- Regular practice of mindfulness or gentle yoga;
- Body relaxation activities: guided meditation, self-massages, hot baths.
The osteopath can also work on the neurovegetative system , using cranial or visceral techniques aimed at calming the general terrain.
Empowering the patient: a key role of the osteopath
One of the objectives of osteopathy is to help the patient regain confidence in their body , understand its signals and develop an active prevention posture.
This can be done through:
- Personalized exercise sheets ;
- Dietary advice for chronic inflammation;
- Invitations to express bodily and emotional feelings , particularly in the case of pain related to the intimate sphere.
Case Studies: Patient Journeys and Positive Responses to Osteopathy
To illustrate the real-world impact of genitofemoral neuralgia and the potential benefits of well-executed osteopathic care, here are three fictional cases inspired by situations frequently encountered in the practice. These stories demonstrate how a comprehensive and individualized manual approach can transform the patient’s experience.
Case 1 – David, 42 years old: Testicular pain after inguinal surgery
Background :
David presented with persistent right groin pain radiating to the testicle, occurring three months after inguinal hernia surgery. He described burning, hypersensitivity to clothing, and discomfort when sitting for long periods. Medical examinations revealed no organic abnormalities, and a neurologist suggested genitofemoral neuralgia.
Osteopathic approach :
The examination reveals significant tension in the inguinal ligament and psoas muscle, as well as a loss of mobility in the lower lumbar region. The osteopath works on post-surgical adhesions , releases the abdominal fascia and relaxes the psoas region. Gentle mobilizations are also performed at the L1-L2 junction.
Result :
After four sessions spaced over two months, David’s pain significantly decreased, allowing him to resume light physical activity. He is now independent, incorporating breathing and stretching exercises into his routine. He describes a notable improvement in his overall well-being.
Case 2 – Michel, 65 years old: Chronic pelvic pain and associated anxiety
Background :
Michel has suffered for several years from diffuse pain in his left inguinal region, radiating to his thigh. Several drug treatments and tests have had no lasting effect. The pain is fluctuating but pervasive, and Michel reports increasing anxiety about his health.
Osteopathic Approach :
The osteopath identifies significant tension in the lumbar region and an overall imbalance in the pelvis. Gentle techniques are applied to the diaphragm, lumbar region, and iliopelvic muscles. Cranial work is also performed to soothe the autonomic nervous system .
Result :
Michel doesn’t see a complete disappearance of pain, but a significant improvement in his daily comfort. He’s walking again, sleeping better, and his anxiety is decreasing. He especially emphasizes the benefits of osteopathy’s humane, non-invasive, and progressive approach .
Conclusion: Towards a More Humane Recognition of Pelvic Pain
Genitofemoral neuralgia remains a condition that is too often misunderstood, underdiagnosed, and poorly managed, particularly because it affects a body region with a high emotional, symbolic, and social significance. However, its repercussions are very real, profound, and debilitating: persistent pain, discomfort in the simplest movements, impact on intimate and social life, feelings of isolation or incomprehension.
Through this article, we wanted to highlight the complexity of this pathology , both on an anatomical and functional level, and above all the richness of a global, integrative approach that respects the experience of each patient.
A multifactorial condition, a multidimensional response
The causes of genitofemoral neuralgia are varied: surgical, mechanical, inflammatory, postural, and even emotional. As a result, the therapeutic response cannot be reduced to a single or linear solution. It requires a cross-disciplinary approach , attentive listening, and constant adaptation to the profile of each patient.
Diagnosis relies as much on clinical skill as on the careful exclusion of other pathologies. It requires time, precision, but above all a desire to understand what is not easily seen . This is also where the role of the osteopath takes on its full meaning.
Osteopathy: support, relief, reintegration
The osteopathic approach seeks not only to eliminate pain, but to restore the body’s overall balance. It acts on:
- local or remote mechanical restrictions that maintain compression;
- muscular and fascial tensions linked to stress or trauma;
- the autonomic nervous system , often disturbed in chronic intimate pain;
- and bodily sensation , the key to sensory reappropriation.
By offering individualized, progressive support that respects the body’s rhythm, osteopathy offers a valuable response to those who suffer from invisible pain, often silenced or trivialized.
Rethinking the therapeutic relationship
The management of genitofemoral neuralgia also invites us to reflect on the therapeutic stance : what do we do when the patient has no visible lesions, but is suffering deeply? How do we listen to them? How can we value their subjective experience, their intuition, their bodily memory?
Acknowledging pain is already a source of relief. Offering a welcoming space for the body can sometimes pave the way for a transformation far greater than the mere disappearance of a symptom.
An opening towards autonomy and prevention
Beyond immediate relief, it is essential to provide patients with tools so that they can become active participants in their own well-being . Posture, breathing, appropriate exercises, healthy lifestyle, emotional expression… These simple but powerful levers can strengthen the body’s resilience and prevent recurrence.
It is with this in mind that osteopathy is a complementary pillar of sustainable health , in conjunction with other professionals (doctors, physiotherapists, psychologists, sexologists, etc.).





")











{kind=link}