

Introduction to Slipped Femoral Capital Epiphysis (SFCE)
Slipped Femoral Capital Epiphysis (SFCE) is one of the most common hip disorders encountered in adolescents, characterized by the displacement of the femoral head relative to the femoral neck at the growth plate. The condition typically occurs during periods of rapid growth, particularly in puberty, when the physis, or growth plate, is structurally weaker and more susceptible to shear forces. SFCE is considered an orthopedic emergency because, if left untreated, it can result in significant and irreversible complications, including chronic pain, impaired mobility, and early-onset osteoarthritis of the hip.
Overview of SFCE
SFCE occurs when the femoral head slips or shifts posteriorly and inferiorly in relation to the femoral neck through the growth plate. This slippage disrupts the alignment of the hip joint, leading to biomechanical instability and dysfunction. The condition is often classified as either stable or unstable, with stable slips allowing for some weight-bearing without severe pain and unstable slips causing intense pain and complete loss of function. Understanding this distinction is critical, as unstable slips are associated with a higher risk of complications, such as avascular necrosis (death of bone tissue due to lack of blood supply) of the femoral head.
The underlying etiology of SFCE is multifactorial, with mechanical and hormonal factors contributing to the weakening of the physis. The mechanical factors include obesity, which increases the load on the growth plate, while hormonal factors, such as changes associated with puberty, may affect cartilage strength and resilience. The interplay between these risk factors, along with genetic predisposition, creates a complex and challenging clinical picture that requires careful assessment and intervention.
SFCE typically presents with symptoms such as hip, groin, thigh, or knee pain, often making diagnosis challenging, as the pain may refer to locations distant from the hip. Additionally, patients may experience a limp, decreased range of motion, or external rotation of the affected leg. These symptoms can be subtle in the early stages, leading to delays in diagnosis. Given the nonspecific nature of early symptoms, healthcare providers must maintain a high index of suspicion, particularly in overweight or rapidly growing adolescents.
Importance of Early Diagnosis and Treatment
Early diagnosis and timely intervention are crucial in managing SFCE and preventing long-term complications. The earlier the condition is identified and treated, the better the chances of preserving hip function and minimizing joint damage. When diagnosed early, surgical intervention, typically involving the stabilization of the femoral head with pins or screws, can be performed to prevent further slippage. This procedure, known as in situ pinning, is highly effective in halting progression and stabilizing the joint. In cases where SFCE is diagnosed late, however, more complex surgical procedures may be necessary, often with less favorable outcomes.
Delayed or missed diagnoses can have devastating consequences, including the development of avascular necrosis and early osteoarthritis. Avascular necrosis occurs when the blood supply to the femoral head is disrupted, leading to the death of bone tissue and subsequent collapse of the joint structure. This complication can result in severe pain and disability, often necessitating hip replacement surgery at a young age. Additionally, untreated SFCE can lead to significant deformity of the hip joint, further increasing the risk of early-onset degenerative changes.
Therefore, the importance of early recognition and treatment cannot be overstated. Clinicians must be vigilant in assessing adolescents who present with hip or referred knee pain, particularly if they exhibit risk factors such as obesity or a history of endocrine disorders. Comprehensive clinical evaluation, combined with appropriate imaging studies such as X-rays, is essential to confirm the diagnosis and guide treatment decisions. Educating healthcare providers and the public about the signs and risk factors of SFCE can also play a critical role in ensuring timely intervention and optimal outcomes for affected adolescents.
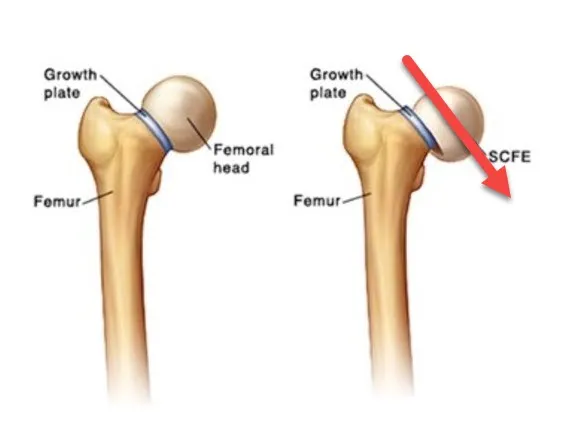
Rapid growth and hormonal imbalance during adolescence can cause the capital femoral epiphysis to slip. An injury or rapid increase in body weight or height can trigger symptoms.

In the first image, an X-ray shows the condition known as Slipped Capital Femoral Epiphysis (SCFE) in an adolescent. The X-ray reveals a displacement of the femoral head relative to the femoral neck, a hallmark of SCFE. The femoral head appears to have slipped backward and downward, indicating the severity of the condition.
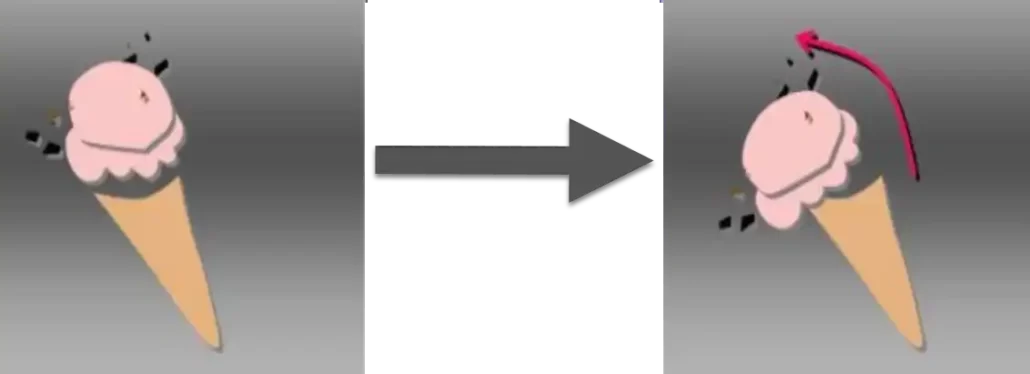
Next to the X-ray, a second image compares this slippage to an ice cream cone, where the ice cream has slipped off the cone. This analogy effectively illustrates the displacement seen in SCFE, making it easier to understand how the femoral head moves out of its normal position, similar to how ice cream might slide off a cone.
⚠️ Important Warning for Readers ⚠️
The information provided in this article about Slipped Capital Femoral Epiphysis (SCFE) is intended for educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or a qualified healthcare provider with any questions you may have regarding a medical condition.
Key Points to Remember:
- Consult a Healthcare Professional: If you or someone you know is experiencing symptoms related to SCFE, such as hip, thigh, or knee pain, seek medical attention immediately.
- Do Not Self-Diagnose: Proper diagnosis and treatment require a thorough evaluation by an orthopedic specialist or healthcare provider.
- Emergency Situations: In cases of severe pain, inability to bear weight, or noticeable limping, do not delay in seeking emergency medical care.
Epidemiology of Slipped Femoral Capital Epiphysis (SFCE)
Slipped Femoral Capital Epiphysis (SFCE) is a pediatric hip disorder that commonly occurs during the adolescent growth spurt, when the femoral head slips off the neck at the growth plate. Understanding the epidemiology of this condition is crucial for early detection, appropriate management, and prevention of long-term complications.
Age and Risk Factors
SFCE typically affects adolescents between the ages of 10 and 16 years, coinciding with periods of rapid skeletal growth and hormonal changes. The growth plate, or physis, is particularly vulnerable during this time because of structural and biochemical transformations that make it susceptible to shear stress. Generally, the peak age of presentation is 12 years for girls and 13.5 years for boys. The condition occurs slightly earlier in females than in males due to the earlier onset of puberty in girls. However, boys are more commonly affected, with a male-to-female ratio of approximately 2:1.
Several risk factors have been associated with SFCE. Obesity is considered one of the most significant, as excessive weight places additional mechanical stress on the already weakened growth plate, increasing the likelihood of a slip. Studies have shown that up to 80% of children diagnosed with SFCE are in the overweight or obese category. In addition to obesity, hormonal imbalances also play a crucial role. Conditions such as hypothyroidism, growth hormone abnormalities, and hyperparathyroidism have been linked to an increased risk of SFCE. Furthermore, genetic predisposition may influence susceptibility, as familial cases of SFCE have been documented, suggesting a hereditary component.
Incidence and Prevalence
The incidence of SFCE varies based on geographic location, ethnicity, and socioeconomic status. It is estimated that the condition affects approximately 10 per 100,000 children annually in the United States. However, the prevalence may be higher in certain populations. For example, studies have shown that SFCE is more common in African American, Polynesian, and Hispanic children compared to their Caucasian counterparts. Conversely, the condition is relatively less frequent among Asian populations. The reasons for these ethnic disparities are not entirely understood but are likely multifactorial, involving genetic, environmental, and socioeconomic influences.
Socioeconomic status has also been implicated as a contributing factor, as children from lower-income families are more likely to be obese, have delayed access to healthcare, and experience nutritional deficiencies, all of which may increase the risk of developing SFCE. Urban areas tend to report higher incidences compared to rural regions, potentially due to lifestyle and environmental factors such as diet and physical activity levels.
Bilateral involvement, where both hips are affected, occurs in 20-40% of cases, often within a year of the initial diagnosis. This highlights the need for vigilant monitoring and follow-up care in patients who present with a unilateral slip. Overall, SFCE is a significant health concern in pediatrics, with its epidemiology underscoring the importance of addressing modifiable risk factors like obesity and ensuring equitable healthcare access across different populations.
Historical Context of Slipped Femoral Capital Epiphysis (SFCE)
Slipped Femoral Capital Epiphysis (SFCE) is a condition that has challenged orthopedic surgeons and pediatricians for over a century. The understanding and treatment of SFCE have evolved considerably, thanks in large part to the work of several key figures in the field of orthopedics. Among them, Sir W. Roger Trethowan stands out as a pioneer whose contributions laid the foundation for modern approaches to SFCE. This historical journey reflects the progress made in diagnosing, managing, and preventing this significant hip disorder.
Contributions of Sir W. Roger Trethowan
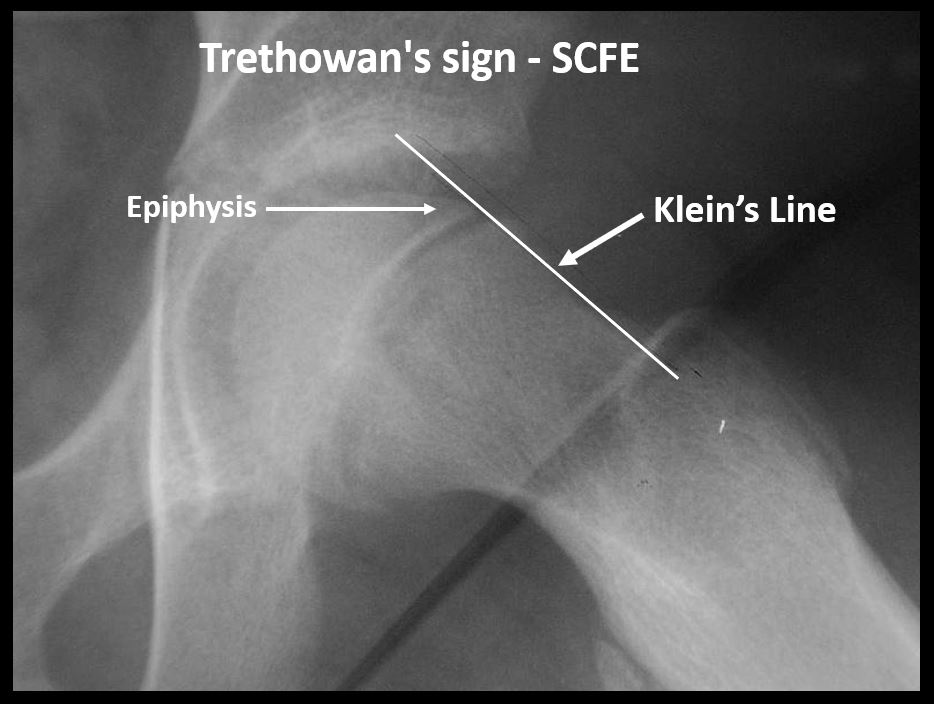
Sir W. Roger Trethowan was a British orthopedic surgeon whose research and clinical observations in the early 20th century significantly advanced the understanding of SFCE. Trethowan is perhaps best known for describing the “Trethowan’s Sign,” a radiographic feature that has become a crucial diagnostic tool in identifying SFCE. This sign involves drawing a line, known as Klein’s line, along the superior edge of the femoral neck on an X-ray. In a normal hip, this line should intersect the lateral aspect of the femoral head. When the line fails to intersect the femoral head, it indicates a possible slip, thus aiding in the early detection of SFCE.
Trethowan’s meticulous studies on the anatomical and mechanical aspects of the hip joint highlighted the importance of growth plate vulnerability during adolescence. His observations emphasized that the femoral head’s slipping was not due to a single cause but rather a complex interplay of mechanical and hormonal factors that weakened the growth plate. Trethowan’s research underscored the necessity of recognizing subtle signs and symptoms to diagnose SFCE early and prevent severe outcomes. His contributions were instrumental in shifting the clinical focus toward early intervention and understanding the biomechanics of the condition.
Trethowan’s work went beyond mere diagnostic advancements. He advocated for the development of standardized surgical techniques to stabilize the femoral head and prevent further slippage. His insights laid the groundwork for the in situ pinning method, which remains a cornerstone of SFCE management today. By emphasizing the need for prompt surgical stabilization, Trethowan helped establish treatment protocols that have saved countless adolescents from debilitating hip deformities and lifelong complications.
Evolution of SFCE Understanding
The understanding of SFCE has undergone significant changes since it was first described in the 19th century. Early medical literature often confused SFCE with other hip pathologies, such as Perthes disease or septic arthritis, due to overlapping symptoms like hip pain and limp. As a result, misdiagnoses were common, and many patients received ineffective or harmful treatments, exacerbating their conditions. It wasn’t until the early 20th century that orthopedic specialists began to distinguish SFCE as a unique and distinct condition.
Trethowan’s contributions, along with advancements in radiographic imaging, revolutionized the diagnosis of SFCE. The development of X-ray technology allowed for more accurate assessments of the hip joint, making it possible to visualize the femoral head’s alignment with the neck and detect early signs of slippage. This breakthrough led to a deeper understanding of the condition’s pathophysiology and the factors contributing to its development, such as the impact of obesity, rapid growth, and hormonal changes during adolescence.
As more cases were studied, researchers recognized that SFCE could be classified into stable and unstable forms, each with different clinical implications and treatment requirements. This classification system has been crucial in guiding treatment decisions and predicting outcomes. In the mid-20th century, further research began to explore the long-term consequences of SFCE, such as the risk of developing early osteoarthritis and avascular necrosis, highlighting the need for early and effective intervention.
The evolution of SFCE management also reflects broader advancements in orthopedic surgery. Early treatments were often rudimentary, ranging from prolonged bed rest to crude traction methods, which frequently failed to prevent further slippage and deformity. With the advent of modern surgical techniques, particularly in situ pinning, the outcomes for patients with SFCE improved dramatically. Surgeons began using pins or screws to stabilize the femoral head, a method that Trethowan had advocated for, preventing additional displacement and preserving the hip joint’s structural integrity.
In recent decades, further research has expanded the understanding of genetic and endocrine factors associated with SFCE. Conditions such as hypothyroidism, growth hormone deficiency, and certain genetic syndromes have been linked to an increased risk of developing SFCE. This new knowledge has allowed for a more comprehensive approach to patient care, incorporating endocrinological assessments and genetic counseling as part of the management strategy.
Today, the legacy of early pioneers like Sir W. Roger Trethowan endures, as his contributions continue to influence the diagnosis and treatment of SFCE. The evolution of SFCE understanding, from its initial misinterpretations to the modern, evidence-based approaches, underscores the importance of ongoing research and collaboration in the field of orthopedics. This historical perspective serves as a reminder of how far medical science has come in addressing this debilitating condition and the importance of continued vigilance in early diagnosis and intervention.

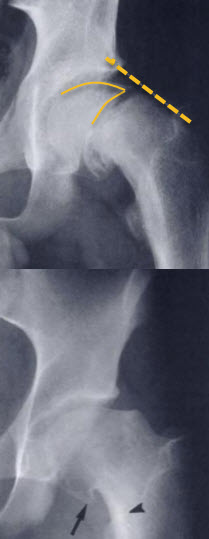
Image Description: Trethowan Sign and Klein Line for Diagnosis of Slipped Capital Femoral Epiphysis (SCFE)
Trethowan Sign:
The image illustrates the Trethowan sign, which is used to diagnose Slipped Capital Femoral Epiphysis (SCFE). In this image, you can see the X-ray of a hip joint where the femoral head appears misaligned with the femoral neck. The normally smooth and continuous curve between the femoral head and neck is disrupted, indicating a positive Trethowan sign. This misalignment suggests that the femoral head has slipped off the neck, a key characteristic of SCFE.
Klein Line:
Next to the Trethowan sign image, the Klein line is demonstrated on another hip X-ray. Klein line is drawn along the superior edge of the femoral neck. In a healthy hip, this line intersects a portion of the femoral head. However, in the image, the Klein line does not intersect the femoral head, or intersects only a small part of it, illustrating the downward slippage of the femoral head seen in SCFE. This deviation from the normal intersection is a critical diagnostic indicator of SCFE.
Together, these images effectively demonstrate the use of Trethowan sign and Klein line in diagnosing SCFE, highlighting the displacement and misalignment of the femoral head relative to the neck.
Pathophysiology of Slipped Femoral Capital Epiphysis (SFCE)
Slipped Femoral Capital Epiphysis (SFCE) is a complex condition primarily affecting adolescents, marked by the slippage of the femoral head relative to the femoral neck at the growth plate, or physis. The pathophysiology of SFCE is intricately related to the structural and biomechanical properties of the hip joint, combined with hormonal and genetic factors that predispose the growth plate to instability. Understanding the mechanisms behind epiphyseal slippage and the anatomy of the hip is crucial for comprehending how and why this disorder occurs.
Mechanisms of Epiphyseal Slippage
The fundamental problem in SFCE is the separation or displacement of the femoral head from the neck through the weakened growth plate. The physis serves as a zone of cartilage that allows for bone elongation during childhood and adolescence. During periods of rapid growth, typically seen in puberty, the growth plate is at its weakest and most vulnerable to mechanical stress. This vulnerability is due to a combination of hormonal influences, mechanical loading, and the intrinsic structural properties of the growth plate.
Several hormonal factors contribute to the weakening of the physis. Puberty brings about a surge in sex hormones, particularly estrogen and testosterone, which play a role in growth plate maturation and fusion. However, during this transitional phase, the cartilage matrix of the physis becomes relatively more pliable and less resilient. Additionally, thyroid hormones and growth hormone, which regulate bone development, may influence the composition and strength of the growth plate. When these hormonal changes coincide with mechanical forces, such as those resulting from increased body weight or physical activity, the growth plate is susceptible to slippage.
Obesity is one of the most significant mechanical risk factors for SFCE. The excess body weight increases the load on the hip joint, exerting shear forces on the growth plate. The femoral head is subjected to considerable stress, especially during weight-bearing activities like walking or running. The combination of these forces and a weakened physis creates an ideal environment for the femoral head to displace. Studies have shown that in obese children, the load on the hip joint can be exponentially greater, compounding the risk of a slip.
Another contributing factor is the relative retroversion of the proximal femur. In some adolescents, the orientation of the femoral head and neck may predispose the growth plate to mechanical instability. The femoral neck may not be perfectly aligned with the femoral head, creating an angle that amplifies shear forces acting on the growth plate. This anatomical variation increases the likelihood of slippage, especially when combined with other risk factors like rapid growth or excessive weight.
Anatomy and Biomechanical Considerations
The anatomy of the hip joint plays a crucial role in the development and progression of SFCE. The hip is a ball-and-socket joint where the femoral head fits into the acetabulum of the pelvis, allowing for a wide range of motion. The femoral neck connects the head to the shaft of the femur, and this structure is crucial for weight-bearing and movement. The physis is located between the head and neck of the femur, and it is this area that is most affected in SFCE.
The physis is composed of cartilage, which is inherently less rigid than bone. It has a unique histological structure with layers responsible for bone growth and elongation. During adolescence, the proliferation and hypertrophy of chondrocytes (cartilage cells) in the growth plate are highly active, contributing to bone growth. However, this same activity renders the physis structurally weaker and more susceptible to mechanical disruption. The chondrocyte organization, along with the extracellular matrix, plays a role in maintaining the structural integrity of the growth plate. When disrupted by external forces, the balance between growth and strength is compromised, leading to slippage.
Biomechanically, the hip joint must bear the body’s weight and absorb the forces generated by movement. The orientation of the femoral neck relative to the shaft, known as the femoral neck-shaft angle, influences how these forces are distributed. In cases where the femoral neck is more horizontally aligned (retroversion), the growth plate experiences increased shear stress. This stress is exacerbated in activities that involve twisting or rotational forces, such as pivoting or sports that require sudden directional changes.
The acetabulum, which forms the socket part of the joint, provides a stabilizing effect, but it cannot fully counteract the forces that lead to slippage if the physis is already weakened. The biomechanics of the hip also involve muscle groups, such as the iliopsoas, gluteal muscles, and adductors, which contribute to the stability and movement of the hip joint. When the femoral head slips, it often results in an externally rotated gait and limited range of motion, as the hip tries to compensate for the misalignment.
The combination of anatomical and biomechanical factors explains why certain individuals are more susceptible to SFCE. Adolescents with poor muscle conditioning, obesity, or anatomical variations are at a higher risk because their hips cannot distribute forces efficiently across the growth plate. Furthermore, genetic predisposition may also influence growth plate strength, making some individuals more vulnerable to the condition.
Causes of upper femoral epiphysiolysis
The exact cause of the slide remains undetermined. It is possible that the displacement is due to a large physiological load, is transmitted through a relatively weak physis. Factors such as obesity increase the weight and mechanical force transmitted, while certain endocrine or renal disorders can promote weakening of the physis. During adolescence, a multitude of factors expose the physis to a high risk of slippage. The femoral head remains in the acetabulum, and the femoral neck moves anteriorly, causing retroversion of the proximal femur. This retroversion results in an analgesic gait marked by external femoral rotation and foot exit. In the absence of bone stability, instability of the epiphysis prevents walking, even with crutches.
Approximately half of patients who develop an unstable sliding femoral epiphysis will develop avascular necrosis of the femoral head later in life.
Intact Ice Cream Cone:
The first image shows an intact ice cream cone, representing a healthy hip joint in a child. The ice cream scoop on top of the cone symbolizes the femoral head, and the cone represents the femoral neck. The region where the scoop meets the cone represents the physis, or growth plate, which is crucial for proper development and alignment.
Ice Cream Slippage:
The second image depicts an ice cream cone with the scoop slipping off, symbolizing Slipped Capital Femoral Epiphysis (SCFE). In this analogy, the slipping ice cream scoop illustrates how the femoral head displaces relative to the femoral neck. Just as the ice cream scoop moves down and off the cone, the femoral head slips downward and backward from the femoral neck, demonstrating the misalignment that occurs in SCFE.
Comparison Explanation:
This visual analogy effectively illustrates the concept of SCFE. The intact ice cream cone represents a healthy hip joint, with the femoral head properly aligned on the femoral neck. The slipping ice cream cone image highlights the displacement that occurs in SCFE, making it easier to understand how the femoral head moves out of position. This comparison helps to visually convey the nature of SCFE in a simple and relatable way.
- Rapid Growth: Superior femoral epiphysiolysis is often associated with periods of rapid growth, typically during puberty. Rapid growth can cause the growth zone (physis) of the femur to become fragile, increasing the risk of slipping.
- Hormonal Factors: Hormonal changes during puberty, particularly increases in growth hormones and sex hormones, may influence bone growth and contribute to the susceptibility of the physis to epiphysiolysis.
- Obesity: Being overweight and obese can increase the load on joints, including the hip, which can potentially increase the risk of epiphysiolysis.
- Genetic Factors: There is evidence to suggest that genetic factors may play a role in the predisposition to upper femoral epiphysiolysis. If family members have had this condition, the risk may be slightly increased.
- Intense Physical Activity: Intense physical activities, especially those involving repetitive movements of the hip, can contribute to epiphysiolysis, especially if associated with rapid growth.
Clinical Presentation of Slipped Femoral Capital Epiphysis (SFCE)
Slipped Femoral Capital Epiphysis (SFCE) is a condition that often presents subtly, making early recognition crucial for effective treatment and prevention of long-term complications. The clinical presentation can vary, but understanding the typical symptoms, warning signs, and stages of SFCE development is essential for healthcare providers, parents, and caregivers.
Symptoms and Warning Signs
The initial symptoms of SFCE can be deceptively mild and nonspecific, often causing delays in diagnosis. The most common symptom is pain, which is usually localized to the hip, groin, or thigh. However, pain may also refer to the knee, making knee pain a frequent but misleading presenting complaint. This referred pain occurs because the obturator nerve, which innervates the hip joint, also provides sensation to the knee, confusing the true source of discomfort. The pain may be intermittent at first, becoming more persistent and severe as the condition progresses. Adolescents often report pain that worsens with physical activity, particularly weight-bearing activities, and improves with rest.
Along with pain, patients may present with a limp or an abnormal gait. The limp is typically an antalgic gait, where the child tries to minimize weight-bearing on the affected side. Parents may notice that the child has difficulty walking or standing for long periods. In severe cases, adolescents may be unable to bear any weight on the affected leg, which is a red flag indicating a more advanced or unstable slip.
Another important sign of SFCE is the external rotation of the affected leg. This may be particularly noticeable when the child is lying down, with the foot pointing outward. The leg may also appear shorter due to the displacement of the femoral head. Limited range of motion, especially restricted internal rotation of the hip, is a consistent finding in SFCE. As the condition worsens, hip flexion and abduction may also become increasingly restricted. Parents might observe that their child struggles with activities like crossing their legs or bending at the hip.
Additionally, adolescents with SFCE may exhibit muscle weakness, particularly in the hip and thigh muscles. This muscle weakness results from reduced activity and the biomechanical changes caused by the slipped femoral head. Over time, the affected side may show signs of muscle wasting or asymmetry compared to the unaffected side.
Healthcare providers should also be aware of less common but significant symptoms, such as a feeling of instability in the hip or a sensation of “locking” or “catching” during movement. These symptoms can indicate more advanced joint involvement and should prompt urgent evaluation.
Stages of SFCE Development
SFCE is typically categorized into stages based on the severity of the slip and the degree of joint involvement. The progression of the condition influences both the clinical presentation and the urgency of treatment.
Acute-on-Chronic Stage:
This stage refers to a sudden worsening of symptoms in a patient who already has a chronic slip. A minor trauma or increased activity can cause an acute exacerbation, leading to severe pain and an inability to bear weight. The previously stable slip may become unstable, and the urgency for surgical intervention increases. Clinically, these patients present with a combination of chronic symptoms and acute exacerbations, often requiring a detailed history to understand the progression.
Pre-Slip or Prodromal Stage:
In the early stage, symptoms may be minimal or absent. Patients may experience vague and intermittent pain in the hip, groin, or knee, often dismissed as growing pains or minor sports injuries. There may be slight discomfort after vigorous activity, but the symptoms are not yet severe enough to cause significant functional impairment. At this stage, radiographic changes can be subtle, and physical examination findings might only show mild limitations in internal rotation. Early detection is rare but ideal for preventing further slippage.
Acute Stage:
The acute stage of SFCE occurs when the femoral head suddenly slips off the neck, often triggered by minor trauma or increased physical activity. The pain becomes severe and disabling, and the adolescent is usually unable to bear weight on the affected leg. This stage is characterized by an unstable slip, with a high risk of complications like avascular necrosis. The hip may be visibly deformed, and there is a significant loss of hip motion, especially in internal rotation and flexion. The external rotation deformity becomes more pronounced, and the leg length discrepancy may be evident.
Chronic Stage:
The chronic stage is the most common presentation, occurring gradually over weeks to months. Patients have persistent, dull pain that progressively worsens. The limp becomes more pronounced, and there is a clear restriction in hip range of motion. The femoral head slowly displaces from the neck, and the body begins to adapt, often resulting in muscle imbalances and gait abnormalities. The chronic form of SFCE can still be either stable or unstable. Stable slips allow the adolescent to bear weight, albeit with discomfort, while unstable slips do not. The risk of joint degeneration increases as the slip becomes more severe, making early intervention critical.
Greater femoral epiphysiolysis is a condition that commonly occurs in adolescents, especially during puberty, when the femoral head slips out of the upper part of the femur through the growth plate. Here are some common symptoms associated with upper femoral epiphysis:
- Hip or Thigh Pain: Pain is often felt in the hip or thigh area on the affected side.
- Lameness: Due to pain and mobility disruption, the patient may experience lameness while walking.
- Restriction of Movement: There may be a reduction in range of movement at the hip, with difficulty performing certain movements.
- Referred Knee Pain: Pain can sometimes radiate to the knee on the affected side, which can lead to confusion as to the source of the pain.
- Analgesic Approach: To minimize pain, the patient can adopt an analgesic approach, changing the way they walk.
- Groin pain: Pain can also be felt in the groin area, as this is where the femoral head moves.
- Reduced Muscle Strength: Due to pain and limitation of movement, there may be a reduction in muscle strength in the affected leg.
- Discomfort when Sitting or Lying: Certain positions, particularly sitting or lying on your side, may be uncomfortable.
- Chronic or Acute Pain: Pain can be chronic, developing gradually, or acute, occurring suddenly following intense physical activity.
Physical Examination of Slipped Femoral Capital Epiphysis (SFCE)
A thorough physical examination is crucial for diagnosing Slipped Femoral Capital Epiphysis (SFCE), particularly because early detection can significantly impact the patient’s prognosis. Clinicians use a combination of screening tests and detailed examination techniques to identify characteristic signs of SFCE and evaluate the extent of hip dysfunction. Given the subtlety of early symptoms, a high degree of clinical suspicion is often necessary, especially in adolescents presenting with hip, groin, or knee pain and an altered gait.
Screening Tests for SFCE
Screening tests for SFCE are essential tools for identifying the condition in its early stages. One of the most important aspects of a physical exam is assessing the patient’s ability to bear weight. In stable SFCE, the patient can typically bear weight on the affected leg, albeit with some discomfort, whereas in unstable SFCE, weight-bearing is impossible due to severe pain. Observing the patient’s weight-bearing status helps differentiate between stable and unstable slips, a distinction critical for determining the urgency of intervention.
Palpation and general observation of the hip area are also part of the screening process. Clinicians should look for asymmetry in hip or thigh musculature and observe any external rotation of the affected leg, which is a classic sign of SFCE. Additionally, leg length discrepancy may be apparent, with the affected leg appearing shorter. This discrepancy is due to the displacement of the femoral head and is a useful clinical clue.
Detailed Examination Techniques
Detailed examination techniques are used to further evaluate hip function and confirm suspicions of SFCE. One commonly used assessment is Drehmann’s Sign, where the patient’s hip involuntarily externally rotates during passive flexion. This sign is highly suggestive of SFCE and occurs because the slipped femoral head limits normal hip motion, causing external rotation to accommodate the deformity.
Another important aspect of the detailed examination is assessing the range of motion. In patients with SFCE, internal rotation, flexion, and abduction of the hip are often restricted. The loss of internal rotation is one of the earliest and most consistent findings. When the hip is passively moved into flexion, it may rotate externally, limiting the overall mobility of the joint. This limitation is indicative of structural changes in the hip and warrants further investigation.
Pain elicitation tests, such as direct pressure on the anterior hip joint or during movement, can help assess the extent of discomfort and functional impairment. Careful attention should be given to how the patient reacts to different movements, as pain is often referred to the knee, making knee pain a misleading but common symptom of SFCE.
Fabere Patrick Test
The Fabere Patrick Test is another valuable technique in assessing SFCE. The test name comes from the positions of the hip during the examination: Flexion, ABduction, External Rotation, and Extension. The test is performed with the patient lying supine. The examiner places the patient’s leg in a figure-four position by flexing, abducting, and externally rotating the hip, with the ankle resting on the opposite knee. Gentle downward pressure is then applied to the knee of the affected leg while stabilizing the opposite pelvis.

A positive Fabere Patrick Test occurs when the maneuver elicits pain in the hip or groin region, suggesting pathology within the hip joint, such as SFCE. This test is particularly useful in differentiating between hip joint problems and issues related to the sacroiliac joint or the lower back. While the Fabere Patrick Test is not specific to SFCE, a positive result, combined with other findings like restricted internal rotation and an externally rotated gait, strengthens the suspicion of a hip disorder.
Gait Analysis and Range of Motion Assessment
Gait analysis is a critical component of the physical examination for SFCE. Patients often present with an antalgic gait, which is characterized by a shortened stance phase on the affected side due to pain. The affected leg may also be externally rotated during walking, a compensatory mechanism that reduces discomfort. In severe cases, a Trendelenburg gait may be observed, where the pelvis tilts downward on the unaffected side during the stance phase of the affected leg. This occurs due to weakness or dysfunction of the hip abductor muscles, further indicating hip instability.
Assessing the range of motion provides additional insights into hip joint function. As mentioned earlier, internal rotation is typically the most restricted movement, followed by limitations in flexion and abduction. The examiner should carefully document the degree of restriction, as this information is valuable for both diagnosis and monitoring the progression of SFCE. Measuring leg length is also important, as a discrepancy between the two legs can indicate the severity of the slip.
In addition to assessing hip mobility, the examiner should evaluate the strength of the surrounding muscles. Muscle weakness, particularly in the hip abductors, can exacerbate joint instability and contribute to functional impairment. The overall muscle tone and any signs of muscle wasting or asymmetry should be noted, as these may indicate chronic or severe cases of SFCE.
Diagnostic Imaging of Slipped Femoral Capital Epiphysis (SFCE)
Accurate and timely diagnosis of Slipped Femoral Capital Epiphysis (SFCE) is essential for preventing severe complications, such as avascular necrosis and early-onset osteoarthritis. Imaging plays a pivotal role in confirming the diagnosis, assessing the severity of the slip, and guiding treatment decisions. Various imaging modalities are used to evaluate SFCE, with X-rays being the primary tool, complemented by advanced imaging techniques like MRI and ultrasound when necessary.
Radiographic Features
X-ray imaging is the first-line modality for diagnosing SFCE and is crucial in assessing the alignment of the femoral head relative to the neck. The two main X-ray views used are the anteroposterior (AP) view and the frog-leg lateral view. These images allow clinicians to visualize the degree of slippage and any associated deformity.
- Anteroposterior (AP) View: This view provides a frontal image of the pelvis, allowing for the assessment of hip joint symmetry and overall bone structure. Clinicians often look for signs of a widened or irregular physis and assess the positioning of the femoral head relative to the acetabulum.
- Frog-Leg Lateral View: This view is more sensitive for detecting subtle slips and provides a clearer picture of the relationship between the femoral head and neck. The frog-leg lateral view is particularly valuable in visualizing posterior displacement, a hallmark feature of SFCE.
Key radiographic features to look for include:
- Physeal Widening: An early sign of instability at the growth plate.
- Posterior and Inferior Displacement: The femoral head may appear displaced downward and backward relative to the femoral neck.
- Trethowan’s Sign (or Klein’s Line): A diagnostic tool where a line drawn along the superior border of the femoral neck should intersect the lateral portion of the femoral head. If it does not, this indicates a possible slip.
Early and Late X-ray Signs
Early X-ray Signs:
In the initial stages of SFCE, radiographic changes can be subtle and may require a high index of suspicion for detection. The preliminary stage is known as the preslip phase, where characteristic features include widening of the growth plate, irregularity, and blurring of the physeal margins. Additionally, the metaphysis may appear demineralized, contributing to the early radiographic changes observed.
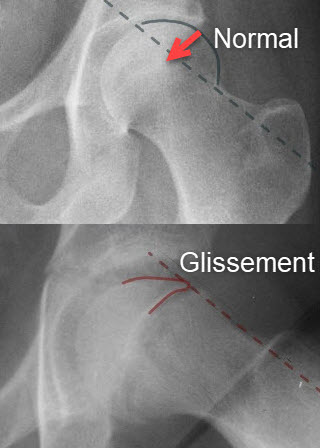
One key indicator in this early stage is the absence of Klein’s line intersection with the femoral head. Trethowan’s line (or Klein’s line) is drawn along the superior border of the femoral neck; in a normal hip, this line intersects the lateral portion of the femoral head. However, in cases of early slippage, the line runs above the femoral head, signaling a potential slip. Furthermore, the lower margin of the metaphysis, which is normally aligned within the acetabulum, may be excluded, indicating early epiphyseal displacement.
Additional signs include a reduction in the depth of the femoral epiphysis and a distinct demarcation between the metaphysis and the epiphysis. Although there may be no obvious deformity at this stage, these minor disruptions in the usual structure of the growth plate highlight the need for careful evaluation, often with the frog-leg lateral view, which is more effective than the AP view in identifying these subtle but significant changes.

Late X-ray Signs:
As SFCE progresses, more pronounced radiographic features become evident. The femoral head may be significantly displaced posteriorly and inferiorly, creating a distinct “step-off” appearance. A key indicator at this stage is the presence of Trethowan’s sign, where the line drawn along the superior border of the femoral neck fails to intersect the femoral head, confirming a substantial slip.
The femoral head often shows signs of atrophy, and the neck angle may decrease to less than 90 degrees, indicating severe slippage and structural deformity. The femoral neck may also appear widened or distorted, accompanied by increased sclerosis of the metaphysis, a phenomenon known as Steel’s metaphyseal whiteness, due to overlapping bone structures. This sclerosis highlights chronic changes and bone remodeling that occur in response to the instability.
Despite these severe changes, the joint space typically remains clear in the early stages of late-phase SFCE, though degenerative changes can develop over time. If left untreated, osteophyte formation and joint space narrowing may occur, signaling the onset of early osteoarthritis. Shenton’s line, an arc formed by the inferior border of the femoral neck and the superior border of the obturator foramen, is often broken, indicating disrupted hip joint alignment. Additionally, in severe cases, the metaphysis of the femur may take on a “bump” appearance, further compromising the hip joint’s normal anatomy and function.
Late signs are often accompanied by bone remodeling and increased sclerosis, particularly around the metaphysis. These changes are indicative of the body’s attempt to stabilize the hip joint, but they also contribute to joint stiffness and limited mobility.
Additional Imaging Modalities
While X-rays are the gold standard for diagnosing SFCE, other imaging modalities are used when additional detail or clarification is needed.
Magnetic Resonance Imaging (MRI):
MRI is highly sensitive and can detect early changes in the physis that may not be visible on X-rays. This modality is particularly useful for identifying pre-slip conditions or early slips in cases where clinical suspicion remains high despite normal X-ray findings. MRI is also valuable for assessing the blood supply to the femoral head, which is critical for predicting the risk of avascular necrosis. The detailed imaging provided by MRI allows clinicians to evaluate cartilage health, bone marrow edema, and subtle structural abnormalities.
MRI is often recommended for patients who have an unclear diagnosis or when there is concern about complications. For instance, in cases of unstable SFCE, MRI can help determine the extent of vascular compromise and guide surgical planning. Additionally, it is an essential tool for follow-up assessments to monitor healing and ensure there is no progression of the slip or development of complications.
Ultrasound:
Ultrasound is less commonly used for diagnosing SFCE but can be helpful in certain cases, especially for assessing joint effusions or soft tissue abnormalities around the hip. It is a non-invasive and radiation-free option that can be particularly useful in younger children or for initial evaluations in emergency settings. However, ultrasound has limited utility in visualizing bone structures compared to X-ray or MRI, and it is generally used as an adjunct rather than a primary diagnostic tool.
Computed Tomography (CT):
CT scans provide high-resolution images of the bone structures and are sometimes used to assess the severity of complex or severe slips. CT imaging can give a three-dimensional view of the hip joint, which is beneficial for surgical planning, especially when precise anatomical details are needed. However, due to the higher radiation exposure, CT is reserved for specific cases where detailed bone imaging is essential.
Differential Diagnosis
- Hip Arthritis: Arthritis of the hip, especially in adults, can cause hip pain and limitation of movement. The key difference is that arthritis is generally associated with progressive wear and tear of the joints, whereas epiphysiolysis is linked to slippage of the femoral head.
- Labral Hip Injuries: Labral injuries can cause similar symptoms, such as hip pain. However, these injuries usually involve damage to the labrum, the cartilage that surrounds the hip joint.
- Legg-Calvé-Perthes disease: This pediatric condition also affects the femoral head, but it is characterized by aseptic necrosis of the femoral head, which results in deformity of the head of the bone.
- Hip Bursitis: Hip bursitis can cause pain and inflammation around the hip joint, but it does not usually involve slippage of the femoral head.
- Hip Fractures: Hip fractures, especially in older adults, can cause pain and limitation of movement. The underlying mechanisms and radiographic features can help differentiate fractures from epiphysis.
- Bone Tumors: Although less common, bone tumors can also cause hip pain. Advanced imaging tests may be needed to evaluate the presence of tumors.
- Hip Infections: Joint infections, although rare, can cause pain and similar symptoms. Laboratory tests and imaging tests can help identify an infection.
Classification of upper femoral epiphysiolysis
Superior femoral epiphysiolysis (SFE) is classically classified according to the severity of slippage of the femoral head relative to the femoral neck. The most commonly used classification is that of Loder , which divides EFS into three categories:
- Stage I – Stable: In this phase, slippage of the femoral head is minimal, and the head remains in contact with the femoral neck. There may be slight asymmetry, but the femoral head has not completely slipped out of its normal position.
- Stage II – Unstable: At this stage, the slippage of the femoral head is greater, and there may be significant displacement relative to the femoral neck. However, the femoral head still remains in contact with the neck.
- Stage III – Dislocation: In this advanced stage, there is complete displacement of the femoral head out of the femoral neck, causing dislocation. The femoral head is no longer in contact with the neck.
This classification is important because it guides the treatment and management of EFS. Stage I patients may benefit from close monitoring and measures to prevent progression. Stage II patients often require surgical intervention, usually in the form of internal fixation to stabilize the femoral head. Stage III patients also require surgery, but treatment may be more complex due to the complete dislocation.
It is essential to note that the Loder classification does not take into account other factors such as the age of the patient, the presence of complications or the severity of symptoms. A comprehensive clinical evaluation, combined with imaging studies, is necessary for appropriate management of upper femoral epiphysiolysis.
Upper femoral epiphysiolysis is classified according to the percentage of slippage:
• Class I: 0% to 33% slip
• Class II: 34% to 50% slip
• Class III: more than 50% slip
Treatment of upper femoral epiphysiolysis
Treatment for EFS depends on the stage of the disease and the severity of the symptoms. Treatment options may include:
- Stage I (Stable): Management may involve close monitoring, activity restrictions, and measures to prevent progression.
- Stage II (Unstable): Most patients in stage II will require surgery to stabilize the femoral head. This may involve internal fixation with screws.
- Stage III (Dislocation): Stage III patients generally require more complex surgery to restore congruence of the femoral head in the neck.
The orthopedic surgeon evaluates the individual case and recommends the best approach based on the severity of the EFS, the patient’s age and other factors. Regular monitoring and post-operative rehabilitation are generally necessary to ensure optimal recovery. Multidisciplinary care, involving orthopedists, physiotherapists and other healthcare professionals, is often crucial to the success of treatment.
Important Notes:
- All exercises should be performed slowly and with control to avoid excessive tension.
- Gradual progression is essential. Start with gentle movements and gradually increase the intensity.
- Listen to your body. If you experience abnormal pain, stop immediately and consult a healthcare professional.
- Professional supervision may be necessary, especially in the early stages of rehabilitation.
Classification Systems for Slipped Femoral Capital Epiphysis (SFCE)
The classification of Slipped Femoral Capital Epiphysis (SFCE) is critical for determining the appropriate treatment approach and predicting long-term outcomes. Various classification systems have been developed to categorize SFCE based on the severity of the slip, clinical presentation, and radiographic findings. These systems help orthopedic surgeons assess the extent of the condition and choose the most effective management strategy.
Grading of SFCE Severity
One of the most widely used systems for grading the severity of SFCE is based on the degree of slippage. The severity is typically divided into three categories: mild, moderate, and severe. These grades are determined by measuring the angle of displacement of the femoral head relative to the neck of the femur, often referred to as the Southwick angle on radiographic images.
- Mild Slippage: The slip angle is less than 30 degrees. Patients with mild SFCE usually experience minimal symptoms, and the hip joint maintains relatively good alignment. Early detection and surgical stabilization are often effective in preventing further slippage and minimizing long-term complications.
- Moderate Slippage: The slip angle ranges from 30 to 50 degrees. This level of slippage typically leads to more pronounced symptoms, including significant pain, restricted hip movement, and an abnormal gait. Moderate SFCE requires prompt surgical intervention to stabilize the femoral head and prevent additional slippage, as well as to reduce the risk of future joint degeneration.
- Severe Slippage: The slip angle is greater than 50 degrees. Severe SFCE often presents with considerable pain, functional impairment, and a high risk of complications, such as avascular necrosis and early-onset osteoarthritis. Complex surgical procedures may be necessary to correct the deformity and stabilize the hip, though the prognosis is generally less favorable than in cases of mild or moderate slippage.
This grading system provides a useful framework for clinicians, as it directly correlates with the urgency of treatment and the likelihood of long-term joint damage. Understanding the severity of the slip helps guide both the surgical approach and the expectations for recovery.
Clinical and Radiographic Classifications
Another important method of classifying SFCE is based on clinical and radiographic criteria. The classification into stable and unstable SFCE is particularly valuable in assessing the risk of complications and determining the immediate treatment strategy.
- Stable SFCE: This classification refers to cases where the patient can still bear weight on the affected leg, even if it is with some discomfort. Stable slips are generally associated with a lower risk of complications, such as avascular necrosis, because the blood supply to the femoral head is less likely to be disrupted. The prognosis for stable SFCE is generally good if treated promptly, and in situ pinning is often sufficient to stabilize the hip and prevent further slippage.
- Unstable SFCE: In these cases, the patient cannot bear weight on the affected leg due to severe pain and dysfunction. Unstable slips are considered orthopedic emergencies, as they are associated with a significantly higher risk of avascular necrosis and other complications. The disruption of the blood supply to the femoral head is a major concern, and urgent surgical intervention is required to minimize damage. The prognosis for unstable SFCE is often poorer, and the risk of long-term joint issues, such as osteoarthritis or femoral head deformity, is higher.
Radiographic Classifications are also used to further evaluate SFCE. In addition to measuring the Southwick angle, X-rays are assessed for signs of physeal widening, posterior and inferior displacement of the femoral head, and changes in the shape of the femoral metaphysis. These radiographic findings help clinicians better understand the extent of the slippage and the potential for future complications.
Advanced imaging techniques, such as MRI, can provide additional insights into the condition of the physis and the blood supply to the femoral head, which is particularly important in cases of unstable SFCE. MRI is also useful for detecting early slips that may not yet be visible on standard X-rays.
Management and Treatment of Slipped Femoral Capital Epiphysis (SFCE)
Managing Slipped Femoral Capital Epiphysis (SFCE) effectively requires a comprehensive approach that includes early diagnosis, appropriate clinical evaluation, timely intervention, and structured post-treatment rehabilitation. The primary goal of treatment is to prevent further slippage of the femoral head and to minimize complications, such as chronic pain and hip deformity, that can lead to long-term disability.
Diagnostic Approach
The diagnostic approach to SFCE begins with a thorough clinical evaluation and is confirmed with imaging studies. Early detection is critical, as the outcome largely depends on the stability of the slip and the timeliness of treatment. Clinicians must maintain a high index of suspicion, especially in adolescents who present with vague symptoms like hip, groin, or referred knee pain, along with a limp.
Clinical Evaluation and Imaging
A detailed history and physical examination are the first steps in evaluating a suspected case of SFCE. Clinicians look for signs such as limited hip range of motion, particularly in internal rotation, and an externally rotated gait. A common clinical test used is the “Drehmann’s sign,” where passive hip flexion causes external rotation of the leg, indicating possible slippage.
If SFCE is suspected, imaging is essential. Anteroposterior and frog-leg lateral X-rays of the pelvis are the standard diagnostic tools. These images can confirm the diagnosis and classify the slip as stable or unstable. In stable slips, patients can still bear weight, albeit with some pain, while unstable slips cause severe pain and loss of function, necessitating urgent intervention. In cases where X-rays are inconclusive or further detail is needed, magnetic resonance imaging (MRI) or computed tomography (CT) scans may be used to assess early slips or evaluate the extent of damage.
Treatment Options
Once diagnosed, the treatment strategy for SFCE depends on the severity and stability of the slip. The primary objective is to prevent further slippage and ensure the femoral head remains aligned within the acetabulum to avoid long-term joint damage.
Surgical and Non-Surgical Interventions
Surgical Treatment: Surgery is almost always the treatment of choice for SFCE, even in stable cases, to secure the femoral head and prevent additional slippage. The most common surgical procedure is in situ pinning, where one or more screws are placed across the growth plate to stabilize the femoral head. This technique is minimally invasive and has a high success rate in halting progression. In cases of severe or unstable slips, more complex surgeries, such as open reduction or realignment procedures, may be necessary. These procedures carry a higher risk of complications, including avascular necrosis and chondrolysis, but are sometimes unavoidable to restore proper hip alignment.
Non-Surgical Treatment: Non-surgical management is rarely an option, as SFCE is a mechanical issue that typically requires stabilization. However, in very early or pre-slip stages, bed rest or traction might be considered to reduce stress on the hip joint while preparing for surgery.
Post-Treatment Rehabilitation
Rehabilitation following surgery is crucial to restoring mobility and function. The initial post-operative phase focuses on pain management and protecting the hip joint. Patients are usually advised to avoid weight-bearing activities for several weeks, depending on the severity of the slip and the surgical procedure performed. Physical therapy plays a pivotal role in this phase, gradually introducing gentle exercises to maintain joint mobility and prevent muscle atrophy.
As healing progresses, rehabilitation efforts shift to strengthening the hip and surrounding muscles, improving balance, and optimizing gait mechanics. The goal is to help patients return to their normal activities while minimizing the risk of further hip problems. Special attention is given to proper body mechanics and posture, ensuring that compensatory movement patterns do not develop.
Exercise, Stretching, and Mobility Restoration
A structured exercise program is essential for regaining full hip function. Low-impact activities, such as swimming and cycling, are recommended to build strength without placing excessive strain on the hip joint. Stretching exercises focus on improving the flexibility of the hip muscles, particularly the iliopsoas and gluteal muscles, which often become tight following surgery. Gradual progression to more challenging exercises, such as weight-bearing and balance training, helps prepare the hip for normal daily activities.
Caregivers and physical therapists guide patients through this process, ensuring exercises are performed correctly to avoid further injury. Proper warm-up and cool-down routines are emphasized, along with modifications to adapt to each patient’s unique recovery timeline.
Long-Term Prognosis and Follow-Up
The long-term prognosis for patients with SFCE varies depending on the severity of the slip and the success of the treatment. Stable slips treated with early surgical intervention generally have good outcomes, with most patients returning to their regular activities. However, those with severe or unstable slips are at a higher risk for complications, such as avascular necrosis, femoroacetabular impingement, or early-onset osteoarthritis.
Regular follow-up appointments are essential to monitor hip development and catch any signs of complications early. Radiographic evaluations are performed periodically to ensure the femoral head remains in place and the growth plate is healing appropriately. Long-term care may involve continued physical therapy, weight management, and lifestyle modifications to reduce the risk of joint deterioration.
Complications and Prognosis of Slipped Femoral Capital Epiphysis (SFCE)
Slipped Femoral Capital Epiphysis (SFCE) is a significant orthopedic condition that, if not properly managed, can result in numerous long-term complications. The prognosis largely depends on the timing of diagnosis, the stability of the slip, and the effectiveness of the treatment. Understanding these potential outcomes is crucial for healthcare providers, patients, and families to prepare for and mitigate the risk of long-term damage.
Potential Long-Term Outcomes
The long-term outcomes of SFCE vary widely based on whether the condition is diagnosed and treated in its early stages. The earlier the intervention, the more favorable the prognosis, as the primary goal of treatment is to stabilize the femoral head and prevent further slippage. When managed promptly, most patients can expect a good outcome, with preserved hip function and minimized joint damage. However, even in cases of successful early intervention, there may be some residual deformity of the femoral head and neck, which can have future implications for hip health.
One of the most common long-term issues following SFCE is femoroacetabular impingement (FAI), where abnormal contact occurs between the deformed femoral head and the acetabulum. This abnormality can lead to joint pain, decreased range of motion, and an increased risk of early-onset hip osteoarthritis. FAI often requires ongoing monitoring and, in some cases, surgical intervention to correct the joint mechanics and reduce symptoms. The severity of this complication typically depends on the extent of the initial slippage and the degree of residual deformity after treatment.
Another possible outcome is leg length discrepancy, which occurs when one leg becomes shorter than the other due to the slippage and subsequent treatment. Although this discrepancy is usually mild, it can contribute to biomechanical imbalances, affecting gait and potentially leading to other musculoskeletal issues over time. Physical therapy and, in some cases, orthotic support or corrective surgery may be necessary to address this complication.
Risk of Osteoarthritis
Osteoarthritis (OA) is a significant long-term complication of SFCE, especially in cases where the femoral head deformity is substantial or when the condition is diagnosed late. The risk of developing OA increases as the hip joint experiences abnormal wear and tear due to irregular joint surfaces and altered biomechanics. Even with early intervention, patients with SFCE are at a higher risk of developing osteoarthritis in adulthood compared to the general population. Studies have shown that approximately 50% of patients with moderate to severe slips may develop hip OA within 20 to 30 years post-treatment.
The early onset of osteoarthritis can severely impact a patient’s quality of life, causing chronic pain, stiffness, and reduced mobility. It may eventually necessitate hip replacement surgery at a relatively young age. Preventive measures, such as maintaining a healthy weight, engaging in low-impact exercises, and avoiding activities that place excessive strain on the hip, can help slow the progression of osteoarthritis. Regular follow-ups with an orthopedic specialist are also crucial for monitoring joint health and managing symptoms as they arise.
Risk of Avascular Necrosis
Avascular necrosis (AVN) of the femoral head is one of the most severe complications associated with SFCE, particularly in cases of unstable slips. AVN occurs when the blood supply to the femoral head is disrupted, leading to the death of bone tissue. This can cause the femoral head to collapse and result in significant joint deformity, chronic pain, and loss of hip function. The risk of AVN is higher in cases where the slip is severe or when there is significant trauma to the hip joint during the slippage or surgical intervention.
Once AVN develops, the prognosis becomes considerably poorer. The treatment options are limited and may include core decompression surgery, bone grafting, or hip arthroplasty (hip replacement). Unfortunately, even with surgical intervention, AVN can lead to a debilitating loss of joint function, requiring ongoing pain management and rehabilitation. The incidence of AVN varies but can affect up to 50% of patients with unstable slips, highlighting the importance of early and careful management to minimize trauma to the hip joint.
Other Complications
In addition to osteoarthritis and avascular necrosis, patients with SFCE may experience chronic pain and reduced hip mobility, even after successful treatment. The altered anatomy of the hip joint can place additional strain on surrounding muscles and tendons, leading to overuse injuries and compensatory patterns of movement. Physical therapy plays a critical role in addressing these issues, focusing on strengthening the hip musculature, improving flexibility, and optimizing gait mechanics to reduce stress on the hip.
Psychological impacts are another consideration, particularly for adolescents who face physical limitations and potential long-term consequences at a young age. Chronic pain and reduced participation in sports or physical activities can affect self-esteem and mental well-being. Support from healthcare professionals, including counseling and mental health resources, can be beneficial for both patients and their families.
Patient Education and Prevention of Slipped Femoral Capital Epiphysis (SFCE)
Slipped Femoral Capital Epiphysis (SFCE) is a serious hip condition that primarily affects adolescents during periods of rapid growth. It can have lasting implications if not identified and treated early. While not all cases can be prevented, understanding the risk factors and taking appropriate preventive measures can greatly reduce the likelihood of developing SFCE. Education for both parents and caregivers is vital in recognizing early warning signs and ensuring prompt medical attention.
Preventive Measures
Although genetic predisposition and hormonal factors that contribute to SFCE are beyond our control, certain modifiable risk factors can be addressed to help reduce the likelihood of slippage. One of the most important measures is maintaining a healthy weight. Obesity is a significant risk factor for SFCE, as the added weight increases the mechanical stress placed on the hip joint and the growth plate. Encouraging a balanced diet and regular physical activity tailored to the child’s needs can help prevent excessive weight gain. Parents should focus on promoting healthy habits from an early age, emphasizing the importance of a nutritious diet rich in fruits, vegetables, whole grains, and lean proteins.
Physical activity is another key preventive measure, though it should be approached with caution. While regular exercise is important for maintaining a healthy weight and promoting bone strength, high-impact sports or activities that put excessive strain on the hips should be avoided, especially if the child is already at risk. Low-impact activities like swimming, cycling, and walking are excellent alternatives that keep children active without placing undue stress on the hip joints.
Additionally, regular check-ups with a pediatrician or family doctor are essential, especially during the adolescent growth spurt. Routine physical examinations can help identify early signs of SFCE or other orthopedic issues. Healthcare providers can monitor growth patterns, weight, and overall development, offering guidance on maintaining musculoskeletal health. For children who have predisposing factors, such as endocrine disorders (e.g., hypothyroidism or growth hormone abnormalities), specialized monitoring may be necessary to ensure early detection and intervention.
Guidance for Parents and Caregivers
Parents and caregivers play a critical role in the early detection and management of SFCE. Awareness of the signs and symptoms is crucial for prompt medical attention. Common symptoms include hip, thigh, or knee pain that may be intermittent or persistent, a noticeable limp, or difficulty bearing weight on one leg. In some cases, children may exhibit an outward rotation of the affected leg or limited range of motion in the hip. Since knee pain is a frequent and misleading symptom, parents should be aware that it may actually originate from the hip.
If any of these signs are present, it is important to seek medical evaluation without delay. Early intervention can significantly improve outcomes, whereas delays in treatment can lead to severe complications, such as avascular necrosis or early-onset osteoarthritis. Educating children about the importance of communicating their discomfort is equally important, as young adolescents may not always express pain clearly or may downplay their symptoms.
Parents should also be mindful of the child’s activity level and provide appropriate support. For example, if a child is overweight, working with a healthcare professional to develop a weight management plan that includes healthy eating and safe physical activities is essential. Open communication with school staff and sports coaches can also be beneficial to ensure that children are not overexerting themselves and that any signs of discomfort are promptly addressed.
Furthermore, families with a history of SFCE or related conditions should inform their healthcare providers, as genetic factors can influence a child’s risk. In cases where a child has an underlying endocrine or metabolic disorder, coordinating care with specialists can help manage and monitor their condition effectively.
Multiple Choice Questions on upper femoral epiphysiolysis
Multiple Choice Questions
- What is superior femoral epiphysiolysis (EFS)? a) Hip fracture
b) Displacement of the femoral head relative to the femoral neck
c) Joint inflammation
d) Genetic bone disease
e) None of the above - Which age group is mainly affected by upper femoral epiphysiolysis? a) Children under 5 years old
b) Adolescents
c) Adults over 50 years old
d) Infants
e) People of all ages equally - What is the most commonly used classification for upper femoral epiphysis? a) Smith’s classification
b) Johnson’s classification
c) Loder’s classification
d) Walker’s classification
e) Brown’s classification - What are the common symptoms of upper femoral epiphysis? a) Hip pain
b) Lameness
c) Restriction of movement
d) All of the above
e) None of the above - Which orthopedic test can be used to evaluate upper femoral epiphysiolysis? a) Hip ultrasound test
b) Fabere (Patrick) test
c) Hip vision test
d) Muscle strength test
e) No test is applicable - Which factor is NOT associated with the risk of upper femoral epiphysis? a) Rapid growth
b) Hormonal factors during puberty
c) Obesity
d) Intense physical activity
e) Aging - What is the recommended treatment for stage II (unstable) upper femoral epiphysis? a) No treatment necessary
b) Anti-inflammatory medications
c) Surgical intervention with internal fixation
d) Physiotherapy alone
e) Regular ice application - What radiographic sign can be observed in upper femoral epiphysiolysis? a) Epiphyseal displacement
b) Shortening of the femoral head
c) Widening of the femoral neck
d) All of the above
e) None of the above - What exercise is recommended for muscle strengthening in the rehabilitation of upper femoral epiphysiolysis? a) Running
b) Hip abduction with elastic band
c) Adductor muscle stretch
d) All of the above
e) None of the above - Why may professional supervision be necessary during upper femoral epiphysis rehabilitation? a) To make the exercises more difficult
b) To ensure safety and effectiveness
c) To reduce treatment costs
d) To speed up the healing process
e) None of the above
Answers to Multiple Choice Questions on upper femoral epiphysiolysis:
- What is superior femoral epiphysiolysis (SFE)? Answer: b) A displacement of the femoral head relative to the femoral neck
- Which age group is mainly affected by upper femoral epiphysiolysis? Answer: b) Adolescents
- What is the most commonly used classification for upper femoral epiphysiolysis? Answer: c) Loder classification
- What are the common symptoms of upper femoral epiphysis? Answer: d) All of the above
- Which orthopedic test can be used to assess upper femoral epiphysiolysis? Answer: b) Fabere test (Patrick)
- Which factor is NOT associated with the risk of upper femoral epiphysiolysis? Answer: e) Aging
- What is the recommended treatment for stage II (unstable) upper femoral epiphysiolysis? Answer: c) Surgical intervention with internal fixation
- What radiographic sign can be seen in upper femoral epiphysiolysis? Answer: d) All of the above
- Which exercise is recommended for muscle strengthening in the rehabilitation of upper femoral epiphysiolysis? Answer: b) Hip abduction with elastic band
- Why may professional supervision be necessary during upper femoral epiphysis rehabilitation? Answer: b) To ensure safety and effectiveness
References
- Mathew SE, Larson AN. Natural History of Slipped Capital Femoral Epiphysis. J Pediatr Orthop. 2019 Jul;39(Issue 6, Supplement 1 Suppl 1):S23-S27. [PubMed]2.
- Loder RT, Skopelja EN. The epidemiology and demographics of slipped capital femoral epiphysis. ISRN Orthop. 2011;2011:486512. [PMC free article] [PubMed]3.
- Wells D, King JD, Roe TF, Kaufman FR. Review of slipped capital femoral epiphysis associated with endocrine disease. J Pediatr Orthop. 1993 Sep-Oct;13(5):610-4. [PubMed]4.
- Perry DC, Metcalfe D, Lane S, Turner S. Childhood Obesity and Slipped Capital Femoral Epiphysis. Pediatrics. 2018 Nov;142(5) [PubMed]5.
- Witbreuk M, van Kemenade FJ, van der Sluijs JA, Jansma EP, Rotteveel J, van Royen BJ. Slipped capital femoral epiphysis and its association with endocrine, metabolic and chronic diseases: a systematic review of the literature. J Child Orthop. 2013 Jun;7(3):213-23. [PMC free article] [PubMed]6.
- Uvodich M, Schwend R, Stevanovic O, Wurster W, Leamon J, Hermanson A. Patterns of Pain in Adolescents with Slipped Capital Femoral Epiphysis. J Pediatr. 2019 Mar;206:184-189.e1. [PubMed]7.
- Georgiadis AG, Zaltz I. Slipped capital femoral epiphysis: how to evaluate with a review and update of treatment. Pediatr Clin North Am. 2014 Dec;61(6):1119-35. [PubMed]8.
- Peck DM, Voss LM, Voss TT. Slipped Capital Femoral Epiphysis: Diagnosis and Management. Am Fam Physician. 2017 Jun 15;95(12):779-784. [PubMed]9.
- Hesper T, Zilkens C, Bittersohl B, Krauspe R. Imaging modalities in patients with slipped capital femoral epiphysis. J Child Orthop. 2017 Apr;11(2):99-106. [PMC free article] [PubMed]10.
- Rebich EJ, Lee SS, Schlechter JA. The S Sign: A New Radiographic Tool to Aid in the Diagnosis of Slipped Capital Femoral Epiphysis. J Emerg Med. 2018 Jun;54(6):835-843. [PubMed]11.
- Mc Cabe A, McArdle S. Towards evidence-based emergency medicine: Best BETs from the Manchester Royal Infirmary. BET 2: Is ultrasound or plain film radiography a more sensitive diagnostic modality for diagnosing slipped capital femoral epiphysis? Emerg Med J. 2014 Jan;31(1):80. [PubMed]12.
- Otani T, Kawaguchi Y, Marumo K. Diagnosis and treatment of slipped capital femoral epiphysis: Recent trends to note. J Orthop Sci. 2018 Mar;23(2):220-228. [PubMed]13.
- Aprato A, Conti A, Bertolo F, Massè A. Slipped capital femoral epiphysis: current management strategies. Orthop Res Rev. 2019;11:47-54. [PMC free article] [PubMed]14.
- Thawrani DP, Feldman DS, Sala DA. Current Practice in the Management of Slipped Capital Femoral Epiphysis. J Pediatr Orthop. 2016 Apr-May;36(3):e27-37. [PubMed]15.
- Davis RL, Samora WP, Persinger F, Klingele KE. Treatment of Unstable Versus Stable Slipped Capital Femoral Epiphysis Using the Modified Dunn Procedure. J Pediatr Orthop. 2019 Sep;39(8):411-415. [PubMed]16.
- Accadbled F, May O, Thévenin-Lemoine C, de Gauzy JS. Slipped capital femoral epiphysis management and the arthroscope. J Child Orthop. 2017 Apr;11(2):128-130. [PMC free article] [PubMed]17.
- Kuzyk PR, Kim YJ, Millis MB. Surgical management of healed slipped capital femoral epiphysis. J Am Acad Orthop Surg. 2011 Nov;19(11):667-77. [PubMed]18.
- Roaten J, Spence DD. Complications Related to the Treatment of Slipped Capital Femoral Epiphysis. Orthop Clin North Am. 2016 Apr;47(2):405-13. [PubMed]19.
- Ganz R. Alshryda S et al. Evidence based treatment for unstable slipped upper femoral epiphysis: Systematic review and exploratory patient level analysis. The Surgeon. 2018; 16: 46-54. Surgeon. 2019 Feb;17(1):61. [PubMed]20.
- Fernandez FF, Eberhardt O, Wirth T. [Early and late complications and their management in slipped capital femoral epiphysis]. Orthopade. 2019 Aug;48(8):677-684. [PubMed]

















{kind=link}