

Introduction
Tennis elbow, or lateral epicondylitis, is a condition that frequently crosses the path of osteopathic practitioners due to its musculoskeletal nature. While the name suggests a sport-related injury, it affects not only tennis players but also individuals engaged in various activities requiring repetitive gripping and wrist extension.
From an osteopathic perspective, tennis elbow often reflects an imbalance or strain within the intricate network of muscles, tendons, and fascia surrounding the elbow joint. Osteopaths recognize that this condition is more than just localized pain; it often signifies underlying dysfunctions in the kinetic chain, extending from the wrist through the forearm, upper arm, and even into the shoulder girdle.
In diagnosing tennis elbow, osteopaths delve beyond the symptoms to uncover contributing factors such as biomechanical imbalances, postural issues, and dysfunctional movement patterns. Through palpation and manual assessment, osteopaths identify areas of tenderness, muscle tightness, and restricted mobility, gaining insights into the root causes of the condition.
Treatment of tennis elbow within an osteopathic framework emphasizes holistic and patient-centered care. Osteopaths employ a range of hands-on techniques to address soft tissue restrictions, improve joint mobility, and restore optimal musculoskeletal function. This may include myofascial release, joint mobilization, muscle energy techniques, and lymphatic drainage to reduce inflammation and promote tissue healing.
In addition to manual therapy, osteopaths guide patients in lifestyle modifications, ergonomic adjustments, and rehabilitative exercises tailored to their specific needs. By empowering individuals to take an active role in their recovery, osteopaths facilitate long-term healing and resilience against future injuries.
Furthermore, osteopathic principles emphasize the interconnectedness of the body, recognizing that disturbances in one area can reverberate throughout the entire system. Therefore, in treating tennis elbow, osteopaths consider the holistic picture, addressing not only the local symptoms but also underlying dysfunctions and compensatory patterns elsewhere in the body.
Through a comprehensive and integrative approach, osteopathic practitioners aim not only to alleviate pain and discomfort but also to enhance overall health and well-being. By restoring balance and harmony within the musculoskeletal system, osteopaths support their patients in achieving optimal function and vitality, both on and off the court.
Understanding Lateral Epicondylitis of the Elbow
Although tennis and other racquet sports are often associated with epicondylitis, several other physical activities can also trigger this condition. The muscles, ligaments and tendons that hold the elbow joint together are essential in this context. The mechanism underlying this injury is repetitive dorsiflexion movements of the wrist in supination and pronation, leading to overuse of the forearm extensor tendons. This continuous stress leads to micro-tears, collagen degeneration and angiofibroblast proliferation.
The natural course of lateral epicondylitis, in the absence of treatment, is characterized by an average duration of 6 to 24 months. Initially considered an inflammatory condition, the understanding of epicondylitis has evolved toward a degenerative perspective. Thus, the term “tendinosis” is now preferred to “tendinitis” to describe this condition, emphasizing the degenerative rather than inflammatory nature of the process.
Underlying Mechanisms of Epicondylitis
Epicondylitis, encompassing both lateral epicondylitis (tennis elbow) and medial epicondylitis (golfer’s elbow), represents a spectrum of overuse injuries affecting the tendons near the elbow joint. While they manifest in different areas, the underlying mechanisms share similarities and complexities. Understanding these mechanisms is crucial for effective management and prevention of these conditions.
The tendons affected in epicondylitis are essential for the movement and stability of the elbow joint. In lateral epicondylitis, the extensor tendons of the forearm, particularly the extensor carpi radialis brevis, attach to the lateral epicondyle of the humerus. Conversely, in medial epicondylitis, the flexor tendons, including the pronator teres and flexor carpi radialis, attach to the medial epicondyle. These tendons play a crucial role in wrist and hand movements, including gripping, lifting, and wrist extension or flexion.
The primary cause of epicondylitis is repetitive stress and overuse of the tendons, leading to microtrauma, inflammation, and eventual degeneration. Activities that involve repetitive gripping, wrist movements, or forceful exertions, such as sports (e.g., tennis, golf), manual labor, and certain occupations (e.g., carpentry, plumbing), are common triggers for these injuries. Additionally, poor biomechanics, improper technique, muscle imbalances, and inadequate recovery can exacerbate the risk of developing epicondylitis.
Microscopic examination of tendon tissue in epicondylitis reveals a cascade of pathological changes, including collagen degeneration, disorganization, and neovascularization. The initial phase involves tendon microtrauma and inflammation, characterized by the release of inflammatory mediators, such as prostaglandins, cytokines, and growth factors. This inflammatory response recruits immune cells to the site of injury, contributing to tissue damage and pain perception.
As the condition progresses, chronic repetitive stress leads to tendon degeneration and fibrosis, altering the structural integrity and biomechanical properties of the tendon. Collagen fibers become disorganized, and the tendon matrix undergoes remodeling, resulting in decreased tensile strength and increased susceptibility to further injury. Neovascularization, or the formation of new blood vessels, is a hallmark feature of chronic tendon pathology and may contribute to persistent pain and inflammation.
Beyond the local tissue changes, epicondylitis is also influenced by systemic factors, including age, genetics, hormonal fluctuations, and metabolic conditions. Tendon tissue becomes less resilient with age due to decreased collagen synthesis and repair capacity, predisposing older individuals to degenerative tendon disorders like epicondylitis. Genetic predisposition may also play a role in determining an individual’s susceptibility to tendon injuries and response to treatment.
Hormonal factors, such as estrogen and testosterone, have been implicated in tendon health and repair processes. Fluctuations in hormone levels, as seen in women during pregnancy or menopause, may influence tendon biomechanics and susceptibility to injury. Metabolic conditions such as obesity, diabetes, and dyslipidemia can contribute to chronic inflammation and impaired tissue healing, further exacerbating the risk of developing epicondylitis.
Lateral epicondylitis of the elbow originates from a complex combination of repetitive movements and pathophysiological mechanisms that challenge the tendons and muscular structures on the outside of the elbow. Understanding these mechanisms is essential to pinpoint the underlying causes of this painful condition.
- Repetitive wrist and hand movements: Lateral epicondylitis is often associated with activities involving repetitive wrist and hand movements. This can include gestures such as grasping objects, rotating the wrist, manipulating tools, and even playing certain sports like tennis. These repeated actions create excessive tension on the tendons attached to the lateral epicondyle, leading to progressive wear and microtrauma.
- Tendon overload and microtrauma: The tendons attached to the lateral epicondyle are subjected to significant stress during repeated movements. Over time, this tendon overload can cause microtrauma to the extensor tendons of the wrist and hand. These micro-lesions activate the body’s inflammatory response, leading to inflammation of the tendons and surrounding structures.
- Vascular alterations and tendon degeneration: Repetitive microtrauma can impair blood circulation in the area, compromising the tendon’s ability to regenerate effectively. This leads to tendon degeneration, characterized by structural changes in the tendon tissues. These structural alterations weaken the tendons and make them more susceptible to damage.
- Inflammatory Response and Persistent Pain: Inflammation is a natural reaction of the body to injury or irritation. In the case of lateral epicondylitis, repeated microtrauma triggers an inflammatory response which, over time, can become chronic. This persistent inflammation contributes to the pain, tenderness, and other symptoms associated with lateral epicondylitis of the elbow.
In summary, lateral epicondylitis of the elbow results from repetitive movements that cause tendon overload, microtrauma, vascular alterations and tendon degeneration. The resulting inflammatory response contributes to the pain characteristic of this condition. A thorough understanding of these mechanisms helps guide treatment approaches toward reducing repetitive strain, promoting tendon healing, and managing inflammation.
Causes of Lateral Epicondylitis of the Elbow
One primary cause of lateral epicondylitis is repetitive strain on the extensor tendons of the forearm. Activities that involve repetitive gripping, twisting, or lifting can place excessive stress on these tendons, leading to microtears and inflammation. For instance, frequent use of a screwdriver, hammer, or computer mouse can contribute to the development of tennis elbow over time.
Furthermore, sports and recreational activities that involve repetitive arm movements can also increase the risk of lateral epicondylitis. While tennis is a common culprit due to the repetitive swinging of the racquet, other sports such as golf, racquetball, and swimming can also strain the forearm tendons and predispose individuals to this condition. Even activities like gardening or painting, which require repetitive wrist and forearm movements, can contribute to the development of tennis elbow.
In addition to repetitive motions, poor technique or form during activities can exacerbate the risk of lateral epicondylitis. Improper gripping or swinging techniques in sports like tennis or golf can place undue stress on the tendons of the elbow, increasing the likelihood of injury. Similarly, using tools or equipment with improper ergonomics or grip size can contribute to overuse and strain on the forearm muscles, leading to the development of tennis elbow.
Individual factors such as age and fitness level can also influence the risk of developing lateral epicondylitis. While this condition can affect individuals of any age, it is more common in adults between the ages of 30 and 50, as tendons become less flexible and resilient with age. Moreover, individuals who are overweight or have poor muscle strength and flexibility may be more susceptible to overuse injuries like tennis elbow due to the increased strain placed on the musculoskeletal system.
Lastly, previous injuries or underlying conditions may predispose individuals to lateral epicondylitis. A history of elbow trauma or overuse injuries, such as repetitive stress from work or sports, can weaken the tendons and make them more susceptible to inflammation and injury. Additionally, certain medical conditions such as arthritis or nerve compression syndromes can affect the stability and function of the elbow joint, potentially increasing the risk of developing tennis elbow.
- Repetitive movements: The most common cause of lateral epicondylitis of the elbow is excessive or repetitive use of the extensor muscles of the wrist and fingers. This can occur in people who frequently engage in activities that involve rotating movements of the wrist, such as tennis (hence the name “tennis elbow”), golf, DIY, or other work activities requiring intensive use of the arm.
- Age: Age can be a risk factor. Lateral epicondylitis of the elbow usually affects people between the ages of 30 and 50, although it can occur at any age.
- Overuse: Repetitive activities or excessive use of the forearm and elbow muscles, without an adequate recovery period, can contribute to the development of this condition.
- Incorrect technique: Improper technique when playing sports or performing manual tasks can increase stress on muscles and tendons, contributing to inflammation.
- Occupational factors: Certain occupations, such as those involving repetitive wrist movements, vibration, or poorly fitted tools, may increase the risk of developing lateral epicondylitis of the elbow.
- Anatomical factors: Anatomical abnormalities, such as a predisposition to increased tension on the tendons, may also play a role in the development of this condition.
- Lack of fitness: A general lack of fitness can weaken the muscles of the forearm, increasing the risk of injuries, including lateral epicondylitis of the elbow.
Symptoms of Lateral Epicondylitis of the Elbow
Lateral epicondylitis, commonly known as tennis elbow, presents with a constellation of symptoms that typically develop gradually over time. Central to these symptoms is pain, which manifests around the outer aspect of the elbow and may radiate down the forearm. This pain is often exacerbated by activities involving gripping or wrist movement, such as lifting objects, shaking hands, or turning a doorknob. Tenderness is also a prominent feature, particularly when pressure is applied to the bony bump on the outside of the elbow. Alongside pain and tenderness, individuals with lateral epicondylitis may experience stiffness in the elbow joint, especially after periods of rest, which can improve with movement but may recur with inactivity. Weakness in the forearm muscles is another common symptom, affecting grip strength and interfering with daily activities. Painful wrist extension against resistance or pronation aggravates symptoms, further highlighting the impact on functional movements. In more severe cases, individuals may even experience pain at rest, disrupting sleep and causing discomfort throughout the day. While swelling is less common, some may notice mild swelling around the elbow joint, often accompanied by warmth and redness. Recognizing these symptoms is crucial for seeking timely medical attention and initiating appropriate treatment to alleviate pain, restore function, and prevent further progression of lateral epicondylitis. Early intervention, including rest, activity modification, and physical therapy, can significantly improve outcomes, while corticosteroid injections or surgery may be necessary in more severe or refractory cases.
- Pain on the outside of the elbow: Pain is usually felt on the outside of the elbow, near the lateral epicondyle. This pain may be mild at first and gradually get worse over time.
- Pain that worsens with activity: Pain often increases with activities that involve grabbing, gripping, twisting the wrist, or any repetitive movement of the forearm. This can include activities like tennis, golf, crafts, or even just lifting objects.
- Grip weakness: Some individuals may experience grip weakness or difficulty holding objects due to pain and associated muscle weakness.
- Stiffness: Stiffness in the elbow may be felt, particularly after a period of inactivity or upon waking up in the morning.
- Pain when turning the wrist: Pain may also be present when turning the wrist or performing twisting movements.
- Tenderness to touch: The lateral epicondyle may be tender to touch, and palpation of this area may cause pain.
- Pain when carrying heavy objects: Pain may be exacerbated when carrying heavy objects or when performing certain daily activities, such as lifting grocery bags.
- Nighttime pain: Some individuals may experience pain during the night, which can disrupt sleep.
Differential diagnoses of Lateral Epicondylitis of the elbow
- Medial epicondylitis (golfer): An inflammation of the tendons on the inside of the elbow, associated with activities that involve rotation of the wrist and arm, such as golf.
- Elbow bursitis: An inflammation of the synovial sac (bursa) located near the elbow, which can cause pain similar to that of epicondylitis.
- Elbow Arthritis: Inflammation of the elbow joints, often associated with autoimmune diseases such as rheumatoid arthritis.
- Elbow instability: Problems with ligaments or joint stability can cause pain and a feeling of weakness.
- Cubital tunnel syndrome: Compression of the ulnar nerve on the inside of the elbow, causing symptoms such as pain, numbness, and tingling in the hand and fingers.
- Stress Fracture: A small fracture due to overuse or repeated stress on the elbow bone.
- Elbow infection: An infection in or around the elbow joint can cause pain and swelling.
- Bone or soft tissue tumors: Although less common, tumors can cause symptoms similar to lateral epicondylitis of the elbow.
Pathophysiology of Lateral Epicondylitis of the Elbow
Lateral epicondylitis, commonly known as tennis elbow, originates from a complex interplay of mechanical strain, microtrauma, and inflammatory responses within the tendons of the forearm muscles. The condition primarily affects the extensor carpi radialis brevis (ECRB) tendon, attaching to the lateral epicondyle of the humerus. Repeated and forceful movements such as wrist extension, along with forearm pronation and supination, place excessive stress on the ECRB tendon, resulting in microscopic tears and damage. This continual microtrauma overwhelms the tendon’s ability to repair itself, leading to a degenerative process marked by disorganized collagen formation and inflammation. Compounded by reduced blood supply to the tendon-bone interface, the inflammatory cascade attracts immune cells, which further contribute to tissue degradation. Additionally, neurogenic inflammation may exacerbate pain perception and disability. Over time, these factors lead to structural changes within the tendon, including fibrosis and neovascularization, predisposing it to recurrent injury. Recognizing this intricate pathophysiology is crucial for tailoring effective treatment strategies, ranging from conservative measures like activity modification and physical therapy to more invasive options such as injections or surgical intervention in severe cases. A comprehensive approach addressing both mechanical and inflammatory aspects is key to managing lateral epicondylitis and preventing long-term complications.
- Overuse or Microtrauma: Lateral epicondylitis often results from overuse of the forearm muscles and repetitive movements, such as those associated with playing tennis (hence the name “tennis elbow”). Repetitive microtrauma can overload the tendon, leading to damage.
- Mechanical Stress: Activities that involve flexion and extension movements of the wrist, as well as frequent hand grip, generate mechanical stress on the extensor carpi radialis tendon (ERCL tendon), which is often involved in epicondylitis lateral.
- Inflammatory Response: Microtrauma causes an inflammatory reaction in the tendon. This inflammation is characterized by the recruitment of immune cells, such as macrophages, to eliminate damaged cells.
- Pain and Swelling: Inflammation can cause pain at the lateral epicondyle of the elbow. Swelling may also occur due to fluid accumulation in the affected area.
- Alterations in the Extracellular Matrix: Repetitive microtrauma can alter the extracellular matrix of the tendon, leading to degeneration and structural changes. This can lead to a loss of tendon elasticity and strength.
- Scar Tissue Formation: In the healing process, the body can form scar tissue to repair microtears in the tendon. However, excess scar tissue can sometimes lead to stiffness and loss of flexibility.
Risk factors
- Repetitive Activities: People involved in professional or recreational activities requiring repetitive wrist and hand movements, such as constant grasping of objects, handling vibrating tools, or intensive practice of certain sports such as tennis, are more likely to develop lateral epicondylitis of the elbow.
- Manual Professions: Certain professions expose individuals more to repetitive movements and manual efforts, thus increasing the risk. This includes construction workers, craftsmen, mechanics and other occupations involving heavy use of the hands.
- Age and Gender: Lateral epicondylitis of the elbow is more common in people aged 30 to 50. Additionally, men seem to be more affected than women.
- Improper Movement Techniques: Improper use of movement techniques, whether at work or while playing sports, can contribute to the development of this condition. Poor posture, improper movements and incorrect lifting techniques can increase the load on the elbow tendons.
Prevention
- Warm-up and Stretching: Before engaging in intensive physical or work activities, a proper warm-up and specific stretches can help prepare muscles and tendons, thereby reducing the risk of injury.
- Proper Lifting Techniques: By learning and adopting proper lifting techniques, especially when using heavy objects, one can minimize strain on the elbow tendons.
- Rest Frequencies and Variety of Movements: Incorporating regular breaks during repetitive activities and diversifying movements can reduce constant pressure on tendons.
- Muscle Strengthening: An exercise program aimed at strengthening the muscles of the forearm and wrist can help stabilize the elbow and reduce the risk of developing epicondylitis.
- Use of Appropriate Equipment: When participating in sports or physical activities, be sure to use appropriate equipment, such as properly fitted tennis rackets, to minimize strain on the elbow.
- Early Medical Consultation: If symptoms such as pain or tenderness in the elbow appear, seeing a healthcare professional as soon as possible can allow for early diagnosis and appropriate management.
By integrating these preventative practices into the lifestyle, it is possible to significantly reduce the risk of developing lateral epicondylitis of the elbow and maintain the health of the associated tendons and muscles.
Osteopathic Approaches in the Treatment of Epicondylitis
Osteopaths take a holistic approach to treating various musculoskeletal conditions, including lateral epicondylitis of the elbow. Although osteopaths do not directly treat the pathology, their intervention aims to improve mobility, reduce muscle tension and promote general balance of the body to support the healing process. Here is how osteopaths can intervene in the treatment of lateral epicondylitis of the elbow:
- Comprehensive Assessment: Osteopaths begin by performing a thorough assessment to understand the patient’s medical history, daily activities, postural habits and specific symptoms of epicondylitis. This assessment guides them in designing a personalized treatment plan.
- Correction of Joint Dysfunctions: Osteopaths can identify and treat joint dysfunctions in the elbow, wrist, shoulder, and even the neck and spine. By restoring joint alignment and mobility, they aim to reduce pressure on the elbow tendons.
- Myofascial Release: Osteopaths use myofascial release techniques to release tension in surrounding muscles, tendons and fascia. This helps improve blood circulation, reduce inflammation and relieve pain associated with epicondylitis.
- Gentle Mobilizations: Gentle manipulations and mobilizations can be used to restore joint flexibility and improve circulation to the affected area. These techniques aim to stimulate the body’s natural healing process.
- Postural and Ergonomic Advice: Osteopaths often provide advice on ergonomics and posture, whether at work, at home or during physical activities. Simple adjustments in the way a person performs certain tasks can reduce pressure on the elbow and promote faster recovery.
- Exercises and Stretches: Osteopaths may recommend specific exercises and stretches to strengthen the muscles of the forearm, wrist and shoulder, helping to stabilize the elbow and prevent future episodes of epicondylitis.
- Global Approach: Rather than focusing only on the painful area, osteopaths take a global approach by considering the entire body. They seek to identify structural and functional imbalances that could contribute to the symptoms of epicondylitis.
Chapman’s Viscero-Somatic Reflex in the Context of Epicondylitis
The Chapman Viscerosomatic Reflex, developed by Dr. Frank Chapman, is an osteopathic approach that posits that changes in internal organs can be reflected in the musculoskeletal structure and adjacent soft tissues. It is based on the idea that visceral imbalances can influence muscle tone and joint mobility in specific areas of the body.
In the context of lateral epicondylitis of the elbow, the Chapman viscerosomatic reflex could be applied as follows:
- Locating Chapman’s Points: Osteopaths trained in this method identify specific Chapman’s Points associated with relevant internal organs. For lateral epicondylitis, points near the elbow and forearm area could be targeted.
- Palpation and Sensitivity Detection: Chapman’s points are palpated to look for areas of tenderness or abnormal tissue densities. In the case of epicondylitis, particular tenderness or tension around the elbow could be observed.
- Gentle Corrections: If Chapman’s points present abnormalities, osteopaths can use gentle techniques, such as light pressure and mobilizations, to restore balance between the visceral and musculoskeletal system. This could help normalize muscle tone and improve circulation to the affected area.
- Influence on Circulation and the Nervous System: By acting on Chapman’s points, osteopaths aim to influence blood circulation, the autonomic nervous system and immune regulation mechanisms. These effects may help reduce inflammation, promote tissue healing, and relieve symptoms associated with epicondylitis.
- Complementarity with Other Approaches: The Chapman viscerosomatic reflex is often used in addition to other osteopathic techniques and conventional treatments for epicondylitis. It can be part of a holistic approach to treating the condition from multiple angles.
Extensor sweeping massage:

Deep massage of the extensors towards the elbow:
Transverse extensor massage:

Using a compression elbow brace
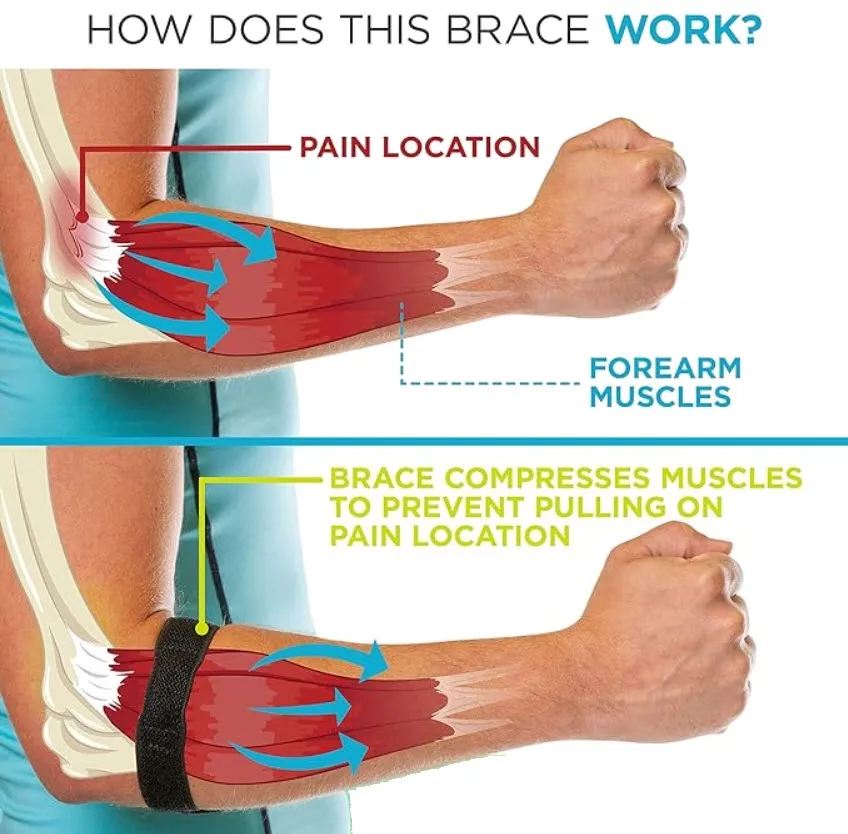
The purpose of the elbow pad is to change the location of the fulcrum. The goal is to reduce the traction tensions on the head of the radius, it will move the location where the elbow pad is located.
Using a compression elbow brace is a common approach to relieving the symptoms of lateral epicondylitis, also known as tennis elbow. Compression elbow support can provide increased support, help reduce inflammation and relieve pain associated with this condition. Here’s how to use a compression elbow brace for lateral epicondylitis:
- Choosing the right size:
- Choosing the right size compression elbow brace is essential to ensure a proper fit. Most elbow pads come in standard sizes, but be sure to follow the manufacturer’s instructions to determine the correct size based on your forearm circumference.
- Correct positioning:
- Place the compression elbow brace around your forearm, just below the elbow. Make sure it fits snugly, but not too tight to avoid discomfort or restriction of blood flow.
- Use during activities:
- Wear the elbow brace during activities that put strain on the elbow, such as playing sports, handling heavy objects, or any other activity that is potentially stressful to the elbow tendons.
- Use during rest:
- It may be beneficial to wear the elbow brace even while resting, especially if pain persists. This can help maintain consistent compression on the affected area and aid recovery.
- Withdrawal for the night:
- It is generally recommended to remove the elbow brace overnight to allow the skin to breathe and avoid prolonged discomfort.
- Combination with other treatments:
- The compression elbow brace can be used in combination with other treatment approaches, such as ice, stretching, and muscle strengthening exercises. Consult a healthcare professional to develop a comprehensive treatment plan.
- Adjustment in case of discomfort:
- If you experience discomfort, numbness, or a tingling sensation, adjust the elbow brace to avoid excessive compression. Make sure it remains comfortable while providing effective support.
Although using a compression elbow brace can be helpful in relieving symptoms of lateral epicondylitis, it is important to consult a healthcare professional for an accurate diagnosis and recommendations tailored to your situation. The compression elbow brace should not be considered a substitute for comprehensive treatment and medical advice.
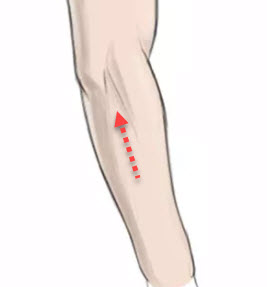
How to wear it
- Bring the arm into extension.
- Carefully observe the muscle that contracts near the elbow.
- It is this muscle that is the source of the discomfort.
- Place the elbow pad about 2 cm downstream (towards the hand)
- It should be placed on the muscle bulge during muscle contraction of the wrist and finger extensors.

Do not wear at night
Using a wrist splint
This splint will aim to limit the extension movement of the arm so that the tendinitis can heal as quickly as possible.
Using a wrist splint can be beneficial in different situations, including for problems such as lateral epicondylitis. However, it is important to note that lateral epicondylitis affects the elbow, not the wrist. If you are referring to another condition or using the wrist splint in the context of epicondylitis, here are some general tips on its use:
- Medical consultation :
- Before using a wrist brace, consult a healthcare professional to obtain an accurate diagnosis of your condition. It is essential to understand the nature of the problem and obtain specific advice on the appropriate type of splint.
- Choice of splint:
- There are different wrist braces on the market, each designed to meet specific needs. Make sure you choose a splint that provides appropriate support to the affected area and is suitable for your condition.
- Proper fit:
- Make sure the splint fits correctly. It should offer support without being too tight, so as not to restrict blood circulation. Follow the manufacturer’s instructions or seek help from a healthcare professional for optimal fit.
- Use during activities requiring the wrist:
- Wear the wrist brace during activities that stress the affected area. This may include repetitive movements, heavy loads or gestures that aggravate the condition.
- Extended Wear:
- Depending on the nature of the condition, you may be required to wear the wrist brace for certain periods of time, including while resting. Follow the recommendations of your healthcare professional.
- Removal for mobility and circulation:
- Remove the splint periodically to allow the skin to breathe and to perform gentle mobility exercises, unless your healthcare professional recommends continued wear.
- Combination with other treatments:
- The use of the brace can be combined with other treatment approaches, such as physical therapy, strengthening exercises, stretching, and appropriate treatment modalities.

Stretching
Stretching is an exercise that aims to improve flexibility, prevent injury, and promote muscle recovery. For lateral epicondylitis of the elbow, targeted stretches can help release muscle tension in the elbow, wrist and forearm area. Here are some helpful stretches:
1. Wrist Extensor Stretch:
- Extend your arm in front of you with your palm facing down.
- Use your opposite hand to gently pull your fingers upward, stretching the wrist extensors.
- Hold the position for 15 to 30 seconds.
- Repeat on the other side.
2. Wrist Flexor Stretch:
- Extend your arm in front of you with your palm facing up.
- Use your opposite hand to gently pull your fingers down, stretching your wrist flexors.
- Hold the position for 15 to 30 seconds.
- Repeat on the other side.
3. Forearm Stretch:
- Extend your arm in front of you, palm down.
- With your opposite hand, bend your fingers down toward the floor, stretching your forearm muscles.
- Hold the position for 15 to 30 seconds.
- Repeat on the other side.
4. Triceps Stretch:
- Raise your right arm above your head.
- Bend your right elbow, bring your right hand behind your head, between your shoulder blades.
- Use your left hand to reach behind your right hand and apply light pressure to stretch the triceps.
- Hold the position for 15 to 30 seconds.
- Repeat on the other side.
5. Shoulder and Trapezius Stretch:
- Place your right hand on your back, with the elbow pointing toward the ceiling.
- Use your left hand to hold your right elbow.
- Gently pull your elbow to the left to stretch the right shoulder and trapezius.
- Hold the position for 15 to 30 seconds.
- Repeat on the other side.
Exercises
Here are some exercises that can help strengthen the muscles of the forearm, wrist and shoulder, while promoting elbow stability. These exercises may be beneficial in the setting of lateral epicondylitis of the elbow, but it is always recommended to consult a healthcare professional before beginning an exercise program, especially if pain persists.
1. Wrist Flexion and Extension:
- Hold a light weight (or water bottle) in your hand, palm facing up.
- Flex the wrist to bring the palm inward.
- Then extend your wrist to bring your palm outward.
- Perform 2 to 3 sets of 15 to 20 repetitions for each wrist.
2. Pronation and Supination of the Wrist:
- Hold a light weight (or water bottle) in your hand with your elbow bent 90 degrees.
- Rotate your wrist so the palm is looking down (pronation), then up (supination).
- Perform 2 to 3 sets of 15 to 20 repetitions for each wrist.
3. Lateral Elevation:
- Hold a light weight in each hand, arms extended at your sides.
- Raise your arms laterally to shoulder height, then lower back down.
- Perform 2 to 3 sets of 12 to 15 repetitions.
4. Elbow Flexion with Dumbbell:
- Hold a dumbbell in your hand, palm facing up.
- Bend your elbow to lift the dumbbell toward your shoulder.
- Slowly lower yourself to the starting position.
- Perform 2 to 3 sets of 12 to 15 repetitions for each arm.
5. Anterior Arm Raise:
- Hold a light weight in each hand, arms extended in front of you.
- Raise your arms to shoulder height, then lower back down.
- Perform 2 to 3 sets of 12 to 15 repetitions.
6. Handshake Exercise with a Rubber Ball:
- Hold a rubber ball in your hand.
- Squeeze the ball as hard as possible for a few seconds, then release.
- Perform 2 to 3 sets of 10 to 15 contractions for each hand.
These exercises aim to strengthen the muscles involved in mobility and stability of the elbow, wrist and forearm. It’s important to start with light weights and gradually increase the resistance over time.
The Evolution of Medical Terminology
The evolution of medical terminology, particularly as it relates to musculoskeletal conditions such as lateral epicondylitis of the elbow, reflects a growing understanding of the nature of the injuries and disease processes. The transition from the term “tendinitis” to “tendinosis” reflects this evolution and has important implications for how the condition is understood and treated.
- Tendinitis vs Tendinosis:
- Tendonitis: Historically, the term “tendinitis” has been used to describe inflammation of the tendon. However, studies have shown that in many cases of tendon conditions, inflammation is not the main feature. Use of the suffix “-itis” implies acute inflammation.
- Tendinosis: The term “tendinosis” is now preferred because it better reflects the chronic and degenerative nature of tendon damage seen in conditions such as epicondylitis. It focuses on structural changes, such as tendon degeneration, rather than acute inflammation.
- Structural Changes and Degeneration:
- Imaging studies and biopsies of tendons affected by conditions such as epicondylitis have shown structural changes, such as microtrauma, alterations in tissue composition, and degeneration rather than active inflammation. The term “tendinosis” more accurately reflects these characteristics.
- Referral to Appropriate Treatments:
- The distinction between tendinitis and tendinosis has important implications for treatment. While traditional approaches for tendinitis may involve managing inflammation, strategies for tendinosis often emphasize activity modification, muscle rehabilitation, tissue strengthening, and approaches to stimulate healing. degenerated tissues.
- Better Clinical Understanding:
- Use of the term “tendinosis” allows healthcare professionals to better understand the chronic and degenerative nature of the condition. This influences the way they approach diagnosis, management and patient counseling, with an emphasis on rehabilitation and prevention of recurrence.
In summary, the transition in terminology from “tendinitis” to “tendinosis” in the context of epicondylitis and other similar conditions reflects a more nuanced understanding of the underlying disease processes. This leads to more tailored treatment approaches, focusing on rehabilitation and long-term management of degenerative changes in tendon tissues.
Screening test
Mills test for lateral epicondylitis (tennis elbow):
- The patient sits or stands with the elbow flexed 90 degrees.
- The practitioner asks the patient to pronounce the wrist (palm down).
- The practitioner applies resistance while asking the patient to extend the wrist against this resistance.
- Pain in the lateral epicondyle during this maneuver may indicate lateral epicondylitis.

It is important to note that the clinical evaluation of epicondylitis may involve several other tests and maneuvers, and the final diagnosis may be made by a healthcare professional, such as a physician, osteopath, or orthopedist.
Conclusion
In conclusion, lateral epicondylitis of the elbow, commonly known as tennis elbow, is a condition that can be debilitating for those who suffer from it. This disorder often results from repetitive movements, putting strain on the extensor tendons of the forearm. Although the term “tendinitis” has long been associated with this condition, modern understanding has reclassified it as “tendinosis”, emphasizing its degenerative rather than inflammatory nature.
Osteopaths play an essential role in the treatment of lateral epicondylitis. Their holistic approach takes into account the underlying mechanisms, risk factors, and offers personalized solutions to relieve pain and promote healing. The use of specific techniques, such as the Chapman viscerosomatic reflex, extensor massage, and the integration of targeted stretches and exercises, offers a comprehensive approach to treating this condition.
It is crucial to recognize early symptoms, such as pain on the outside of the elbow, muscle weakness, and stiffness, in order to seek appropriate treatment in a timely manner. Additionally, prevention plays a key role, educating about risk factors and encouraging healthy habits, including regular breaks from repetitive activities.
By sharing case studies, patient testimonials and exploring the multiple facets of osteopathy in the context of lateral epicondylitis, this therapeutic approach positions itself as a promising solution to relieve pain, restore functionality and improve function. quality of life of individuals affected by this delicate condition.
References
- Welsh P. Tendon neuroplastic training for lateral elbow tendinopathy: 2 case reports. J Can Chiropr Assoc. 2018 Aug;62(2):98-104. [PMC free article] [PubMed]
- Kwapisz A, Prabhakar S, Compagnoni R, Sibilska A, Randelli P. Platelet-Rich Plasma for Elbow Pathologies: a Descriptive Review of Current Literature. Curr Rev Musculoskelet Med. 2018 Dec;11(4):598-606. [PMC free article] [PubMed]
- Patio JM, Horn AR, Michelini A, Abdon I, Ramos Vertiz AJ. Elbow Posterolateral Rotatory Instability due to Cubitus Varus and Overuse. Case Rep Orthop. 2018;2018:1491540. [ PMC free article ] [ PubMed
- Degen RM, Conti MS, Camp CL, Altchek DW, Dines JS, Werner BC. Epidemiology and Disease Burden of Lateral Epicondylitis in the USA: Analysis of 85,318 Patients. HSS J. 2018 Feb;14(1):9-14. [PMC free article] [PubMed]
- Chevinsky JD, Newman JM, Shah NV, Pancholi N, Holliman J, Sodhi N, Eldib A, Naziri Q, Zikria BA, Reilly JP, Barbash SE, Urban WP. Trends and Epidemiology of Tennis-Related Sprains/Strains in the United States, 2010 to 2016. Surg Technol Int. 2017 Dec 22;31:333-338. [PubMed]
- Hassebrock JD, Patel KA, Makovicka JL, Chung AS, Tummala SV, Hydrick TC, Ginn JE, Hartigan DE, Chhabra A. Elbow Injuries in National Collegiate Athletic Association Athletes: A 5-Season Epidemiological Study. Orthop J Sports Med. 2019 Aug;7(8):2325967119861959. [PMC free article] [PubMed]
- Kraushaar BS, Nirschl RP. Tendinosis of the elbow (tennis elbow). Clinical features and findings of histological, immunohistochemical, and electron microscopy studies. J Bone Joint Surg Am. 1999 Feb;81(2):259-78. [PubMed]
- Nirschl RP, Pettrone FA. Tennis elbow. The surgical treatment of lateral epicondylitis. J Bone Joint Surg Am. 1979 Sep;61(6A):832-9. [PubMed]
- Jeon JY, Lee MH, Jeon IH, Chung HW, Lee SH, Shin MJ. Lateral epicondylitis: Associations of MR imaging and clinical assessments with treatment options in patients receiving conservative and arthroscopic managements. Eur Radiol. 2018 Mar;28(3):972-981. [PubMed]
- Ramage JL, Varacallo M. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Aug 30, 2021. Anatomy, Shoulder and Upper Limb, Wrist Extensor Muscles. [PubMed]


















{kind=link}