

Tommy John Ulnar Collateral Ligament Injury, a term now famous in the sports world, has its origins in the demanding field of professional baseball.
Introduction: When the Elbow Cries Out
In the world of sports, certain injuries mark more than just a setback—they become historical turning points, reshaping not only athletic careers but also the very landscape of sports medicine. One such injury is the tear of the ulnar collateral ligament (UCL) of the elbow. Though relatively unknown to the general public, this small ligament on the inner side of the elbow plays a critical role in stabilizing the joint during powerful and repetitive arm movements, particularly in throwing athletes. When it ruptures, it doesn’t just halt a season—it can derail an entire career. But in the case of Tommy John, it also ignited a medical revolution.
Prior to 1974, a torn UCL was often considered a career-ending injury for professional pitchers. That changed with Tommy John, a star pitcher for the Los Angeles Dodgers, who became the first athlete to undergo an unprecedented surgical procedure performed by orthopedic surgeon Dr. Frank Jobe. The idea was bold: reconstruct the damaged ligament using a tendon harvested from elsewhere in the body. The operation was a gamble—but it worked. Not only did Tommy John return to the game, he pitched for many more seasons, and the procedure that now bears his name became a milestone in sports surgery.
Since then, Tommy John surgery has been performed thousands of times, especially among baseball players, with remarkably high success rates. Many athletes even report improved performance after recovery—a paradox that fascinates, but also raises questions. Is surgery becoming a shortcut to enhanced capabilities, rather than a last resort? And more importantly, what are we missing by focusing solely on surgical success?
Beneath the surface of this medical triumph lies a more complex reality. The increasing incidence of UCL injuries, especially among young athletes, reflects deeper issues: early sport specialization, excessive workloads, and year-round competition. The success of Tommy John surgery should not overshadow the importance of prevention, nor the need for a more holistic approach to athlete care. This is precisely where osteopathy can play a pivotal role—both upstream, by identifying and correcting biomechanical imbalances that predispose athletes to injury, and downstream, by supporting rehabilitation and minimizing compensatory strain.
This article offers a comprehensive journey through the world of UCL injury and Tommy John surgery—from the ligament’s anatomical function to the latest surgical techniques, from post-operative recovery to osteopathic support and injury prevention. We will explore how this once career-threatening injury became a symbol of medical innovation—and a topic of ongoing debate.
We’ll also examine the limits of this success story. Though the surgery often yields excellent results, it is not without risk. Recovery is long, recurrence is possible, and the biomechanics of throwing must often be adapted. Osteopaths can be key allies in this process—supporting tissue integration, restoring disrupted functional chains, and offering somatic awareness to athletes who may be pushing their bodies beyond healthy limits.
Ultimately, this article invites a broader reflection: how far can we go in “fixing” the body without truly listening to its signals? Modern surgery has achieved remarkable feats, but healing—in its deepest sense—is not merely mechanical. The UCL tear, like many sports injuries, is also a call to reconsider our training culture, our relationship to performance, and the space we allow for rest, balance, and embodied intelligence.
By taking Tommy John surgery as our point of departure, this article dives into far more than a medical technique. It opens a conversation about the future of athlete care—one where scalpel, osteopathic touch, and human insight work hand in hand.
Baseball pitchers are at high risk for ulnar collateral ligament (UCL) injuries due to the repetitive and forceful motions of throwing. The extreme stress placed on the elbow joint during pitching can cause tears or strains in the UCL, leading to pain, instability, and decreased throwing performance. Over time, this repetitive stress may result in chronic elbow pain and necessitate surgical intervention, such as Tommy John surgery, to repair or replace the damaged ligament. Proper throwing mechanics, strength training, and adequate rest are crucial in preventing UCL injuries and maintaining elbow health.
Functional Anatomy of the Elbow: The Role of the UCL
Understanding the foundation before the fall
The elbow may appear to be a simple hinge joint, but its internal architecture is remarkably complex, especially when examined through the lens of high-performance athletics. Among the many ligaments and stabilizing structures that allow for precision and power in the throwing arm, the ulnar collateral ligament (UCL) plays a starring role. Though small in size, the UCL is monumental in function, particularly for athletes whose careers rely on the repetitive overhead throwing motion, such as baseball pitchers, javelin throwers, and tennis players.
Anatomical Overview
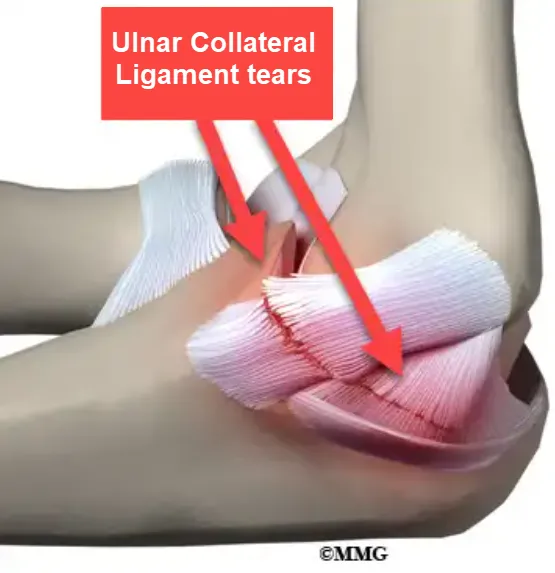
The elbow joint is formed by the articulation of three bones: the humerus (upper arm bone), the ulna, and the radius (the two forearm bones). The UCL, also known as the medial collateral ligament of the elbow, connects the medial epicondyle of the humerus to the sublime tubercle of the ulna. It is comprised of three distinct bands:
- Anterior bundle: The most important and functionally dominant band, especially in resisting valgus stress during throwing.
- Posterior bundle: Engaged primarily when the elbow is flexed beyond 60°.
- Transverse bundle: Offers limited mechanical stability but connects the two parts of the ulna.
Together, these bundles create a strong fibrous structure responsible for resisting medial (valgus) force—exactly the type of stress imposed on the elbow during high-velocity throws.
Biomechanical Function During Throwing
In throwing athletes, the UCL is subjected to extreme forces. During the late cocking and early acceleration phases of a pitch, the elbow rapidly transitions from maximal external rotation of the shoulder into a whip-like extension. This action generates tremendous valgus torque across the elbow joint—often exceeding 60 Nm in professional pitchers. This is near the physiological limit of the UCL’s tensile strength.
The anterior bundle bears the brunt of this load. If the athlete’s neuromuscular control, scapular mechanics, or core stability are even slightly compromised, the ligament is exposed to microtrauma. Over time, this leads to progressive stretching, fraying, and ultimately, rupture.
What’s particularly alarming is that many of these injuries are not the result of one traumatic event, but rather cumulative stress—a slow and silent deterioration caused by thousands of throws over months and years. This chronic degradation can eventually result in a complete tear, especially when combined with factors such as fatigue, poor technique, or insufficient recovery.
Developmental and Structural Vulnerabilities
An important consideration is the age and skeletal maturity of the athlete. In adolescents, the growth plates (physes) around the elbow are still open and more vulnerable to stress than the ligament itself. As a result, young athletes may suffer from medial epicondyle apophysitis (“Little League elbow”) rather than classic UCL tears. However, with increasing specialization and year-round training, UCL injuries are now appearing earlier, even in high school athletes.
Another anatomical factor involves variations in UCL thickness and quality. Some individuals naturally have thinner ligaments, placing them at greater risk. Joint laxity, hypermobility, and hormonal influences may also modulate ligament resilience—especially in female athletes.
The Domino Effect: UCL and the Kinetic Chain
The UCL does not work in isolation. It functions within an intricate kinetic chain that includes the shoulder girdle, thoracic spine, core, hips, and even the feet. If any link in this chain is dysfunctional—such as a weak scapular stabilizer, a stiff thoracic spine, or poor hip mobility—the elbow becomes the site of compensation.
This is where the osteopathic perspective shines. By assessing the global mechanics of the athlete, rather than focusing only on the elbow itself, an osteopath can identify upstream contributors to UCL strain. For example, restrictions in diaphragmatic movement can alter trunk rotation, subtly increasing torque on the elbow with each throw.
The Thrower’s Injury: Mechanisms and Symptoms
When the perfect motion turns destructive
Throwing a ball at over 90 miles per hour may look fluid and effortless, but from a biomechanical standpoint, it is an incredibly violent act—especially for the elbow. For professional and high-level amateur throwers, this motion is repeated hundreds, sometimes thousands of times each season. Over time, even the most finely tuned body can begin to fray under the strain. When the ulnar collateral ligament (UCL) becomes the weak link in this kinetic chain, a cascade begins—one that can quietly progress from minor irritation to full rupture.
A Degenerative Process Before the Tear
Unlike acute injuries that strike suddenly and obviously, UCL damage typically follows a pattern of chronic microtrauma. Each pitch places valgus stress on the elbow, with the anterior bundle of the UCL absorbing most of the tension. If this stress consistently exceeds the ligament’s capacity to recover, tiny tears accumulate. Over weeks, months, or even years, the UCL weakens, loses its elasticity, and eventually gives way.
Certain technical flaws or biomechanical inefficiencies can accelerate this process:
- Excessive shoulder external rotation during the late cocking phase.
- Early trunk rotation, which increases the valgus load on the elbow.
- Scapular instability or weak core engagement, which disrupts force transfer.
These subtle imperfections, repeated thousands of times, shift the burden to the elbow—and the UCL in particular—leading it toward structural failure.
Recognizing the Symptoms
The clinical presentation of a UCL injury varies depending on its severity. However, some hallmark symptoms tend to appear:
- Medial elbow pain, often described as a sharp, burning, or pulling sensation during throwing.
- Loss of velocity and control, particularly during the later innings or repetitions.
- A sense of looseness or instability, as if the elbow “gives out.”
- Clicking or popping sensations during the throw, especially with partial tears.
- Pain at rest or upon palpation, especially along the medial epicondyle.
In younger athletes, the symptoms may be more diffuse and subtle. Pain may mimic general soreness or overuse, leading to misdiagnosis and delayed intervention.
Differential Diagnosis and Diagnostic Challenges
Several conditions can mimic or accompany UCL injuries, making diagnosis challenging:
- Medial epicondylitis (golfer’s elbow): A tendinopathy of the wrist flexors, more superficial and often less debilitating.
- Ulnar nerve entrapment: Produces tingling or numbness in the ring and little fingers.
- Posterolateral rotatory instability: A rare cause of elbow instability seen in hypermobile athletes.
- Posterior impingement syndrome: Causing pain at terminal extension, often confused with medial instability.
For this reason, a thorough clinical evaluation is critical. Valgus stress testing, the moving valgus stress test, and the “milking maneuver” can help isolate UCL involvement. Imaging such as dynamic ultrasound or MR arthrogram provides valuable confirmation.
Why Early Diagnosis Matters
One of the greatest pitfalls in managing UCL injuries is delayed recognition. Too often, medial elbow pain is dismissed as simple fatigue, inflammation, or “just part of the game.” Yet catching the injury early—before a full rupture—opens the door to conservative management through rest, biomechanical correction, and osteopathic care.
From an osteopathic perspective, pain is not an isolated phenomenon. It is a signal of systemic imbalance. The UCL may be the site of failure, but the cause often lies upstream—at the shoulder, the thoracic spine, the pelvis, or even the diaphragm. For instance, restricted rib mobility can impair trunk rotation, subtly altering arm mechanics and overloading the elbow. Similarly, dysfunctions in the sacroiliac joint may disrupt lower-body force transfer, forcing the arm to compensate.
By identifying and addressing these deeper contributors, osteopathy can not only relieve symptoms but help restore balance to the entire kinetic chain—reducing the likelihood of reinjury and supporting long-term performance.
Biomechanics of ulnar collateral ligament (UCL) injury
The biomechanics of an ulnar collateral ligament (UCL) injury of the elbow typically involves overloading or excessive stress on the ligament, leading to changes in the normal forces and motion of the elbow joint. Here is a biomechanical perspective of this injury:
- Elbow Movements: The elbow is a complex joint that allows for several types of movements, including flexion, extension, pronation and supination. These movements are controlled by the coordination of muscles, tendons and ligaments around the joint.
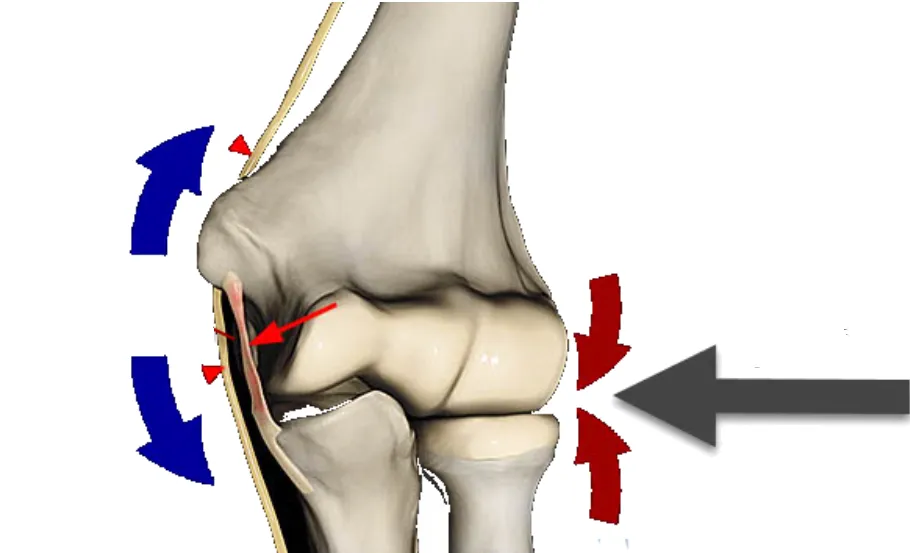
- Role of the ulnar collateral ligament (UCL): The ulnar collateral ligament is located on the inner side of the elbow and contributes to the stability of the joint. It resists the force that can push the elbow outward, helping to prevent excessive opening of the joint on the opposite side (valgus).
- Valgus stress: UCL injury is often associated with excessive valgus stress on the elbow. This typically occurs during activities that involve a throwing or striking motion, where the elbow is under significant load while being flexed.
- Change in joint dynamics: Injury to the UCL can lead to weakening or failure of the ligament, thereby altering normal joint dynamics. This can lead to elbow instability and increased opening on the medial side.
- Muscular compensation: In response to instability, the muscles around the elbow may attempt to compensate by providing increased muscular support. However, this can lead to muscle imbalances and increase the risk of injury.
- Impacts on pronation and supination: The UCL injury can also affect the pronation (inward rotation) and supination (outward rotation) movements of the forearm, as these movements are linked to the stability of the elbow joint.

Valgus elbow strain is a common injury mechanism among elite baseball pitchers like Clayton Kershaw of the Dodgers. The repetitive throwing motion, especially the rapid arm acceleration and deceleration, places significant stress on the ulnar collateral ligament (UCL) on the inside of the elbow. Over time, this strain can lead to microtears, ligament weakening, and ultimately UCL damage, causing pain, instability, and reduced performance. Preventive measures such as biomechanical analysis, targeted strength training, and proper pitching techniques are crucial in protecting the UCL from long-term damage and maintaining a successful pitching career.

The Thrower’s Injury: Mechanisms and Symptoms
When the perfect motion turns destructive
Throwing a ball at over 90 miles per hour may look fluid and effortless, but from a biomechanical standpoint, it is an incredibly violent act—especially for the elbow. For professional and high-level amateur throwers, this motion is repeated hundreds, sometimes thousands of times each season. Over time, even the most finely tuned body can begin to fray under the strain. When the ulnar collateral ligament (UCL) becomes the weak link in this kinetic chain, a cascade begins—one that can quietly progress from minor irritation to full rupture.
A Degenerative Process Before the Tear
Unlike acute injuries that strike suddenly and obviously, UCL damage typically follows a pattern of chronic microtrauma. Each pitch places valgus stress on the elbow, with the anterior bundle of the UCL absorbing most of the tension. If this stress consistently exceeds the ligament’s capacity to recover, tiny tears accumulate. Over weeks, months, or even years, the UCL weakens, loses its elasticity, and eventually gives way.
Certain technical flaws or biomechanical inefficiencies can accelerate this process:
- Excessive shoulder external rotation during the late cocking phase.
- Early trunk rotation, which increases the valgus load on the elbow.
- Scapular instability or weak core engagement, which disrupts force transfer.
These subtle imperfections, repeated thousands of times, shift the burden to the elbow—and the UCL in particular—leading it toward structural failure.
Recognizing the Symptoms
The clinical presentation of a UCL injury varies depending on its severity. However, some hallmark symptoms tend to appear:
- Medial elbow pain, often described as a sharp, burning, or pulling sensation during throwing.
- Loss of velocity and control, particularly during the later innings or repetitions.
- A sense of looseness or instability, as if the elbow “gives out.”
- Clicking or popping sensations during the throw, especially with partial tears.
- Pain at rest or upon palpation, especially along the medial epicondyle.
In younger athletes, the symptoms may be more diffuse and subtle. Pain may mimic general soreness or overuse, leading to misdiagnosis and delayed intervention.
Differential Diagnosis and Diagnostic Challenges
Several conditions can mimic or accompany UCL injuries, making diagnosis challenging:
- Medial epicondylitis (golfer’s elbow): A tendinopathy of the wrist flexors, more superficial and often less debilitating.
- Ulnar nerve entrapment: Produces tingling or numbness in the ring and little fingers.
- Posterolateral rotatory instability: A rare cause of elbow instability seen in hypermobile athletes.
- Posterior impingement syndrome: Causing pain at terminal extension, often confused with medial instability.
For this reason, a thorough clinical evaluation is critical. Valgus stress testing, the moving valgus stress test, and the “milking maneuver” can help isolate UCL involvement. Imaging such as dynamic ultrasound or MR arthrogram provides valuable confirmation.
Why Early Diagnosis Matters
One of the greatest pitfalls in managing UCL injuries is delayed recognition. Too often, medial elbow pain is dismissed as simple fatigue, inflammation, or “just part of the game.” Yet catching the injury early—before a full rupture—opens the door to conservative management through rest, biomechanical correction, and osteopathic care.
From an osteopathic perspective, pain is not an isolated phenomenon. It is a signal of systemic imbalance. The UCL may be the site of failure, but the cause often lies upstream—at the shoulder, the thoracic spine, the pelvis, or even the diaphragm. For instance, restricted rib mobility can impair trunk rotation, subtly altering arm mechanics and overloading the elbow. Similarly, dysfunctions in the sacroiliac joint may disrupt lower-body force transfer, forcing the arm to compensate.
By identifying and addressing these deeper contributors, osteopathy can not only relieve symptoms but help restore balance to the entire kinetic chain—reducing the likelihood of reinjury and supporting long-term performance.logy
The UCL Reconstruction Surgery: Step-by-Step
Precision that gives the throwing arm a second life
Tommy John surgery is not merely a repair—it is a true ligament reconstruction, requiring anatomical precision, surgical finesse, and a deep understanding of throwing biomechanics. Since its groundbreaking debut in 1974, the procedure has evolved considerably, yet its fundamental principle remains the same: replace the damaged ulnar collateral ligament (UCL) with a tendon graft capable of restoring joint stability.
Let’s walk through the key steps of this now-iconic surgical intervention.
1. Preoperative Planning: A Multidimensional Assessment
Before surgery, a comprehensive evaluation is essential to confirm the diagnosis, rule out additional injuries (such as ulnar nerve entrapment or cartilage damage), and plan the most appropriate technique. Imaging—usually MRI or MR arthrography—is crucial.
The surgeon also discusses the choice of graft, expected outcomes, and the demanding rehabilitation process with the athlete, ensuring informed consent and long-term engagement.
2. Graft Selection: Autograft or Allograft
The replacement for the torn UCL is typically a tendon harvested from the patient (autograft), taken from an area of the body where it’s not functionally essential. The most commonly used tendons include:
- Palmaris longus tendon (forearm): A slender tendon absent in about 10–15% of individuals, often chosen for its ideal size and dispensability.
- Gracilis tendon (inner thigh): Preferred if the palmaris longus is absent or a stronger graft is required.
In some cases, an allograft (donor tendon) may be used, particularly for revision surgeries or special circumstances.
3. Surgical Exposure of the Elbow
The patient is placed under general or regional anesthesia, typically lying supine with the arm extended on a side table.
A medial incision is made over the elbow to expose the UCL area. Careful dissection is performed to identify and protect the ulnar nerve, which may be transposed anteriorly depending on the situation.
The native ligament is assessed. If irreparably damaged, it may be removed or left in place to provide biological support for the graft.
4. Bone Tunnel Drilling and Graft Placement
Two small bone tunnels are drilled:
- One in the medial epicondyle of the humerus.
- One in the sublime tubercle of the ulna.
The graft is passed through these tunnels in a figure-eight configuration, simulating the original UCL’s path and tension.
Several techniques exist:
- Jobe’s original figure-eight method.
- Docking technique, allowing precise control over graft tension and positioning.
- Hybrid techniques, incorporating modern anchors or bioabsorbable fixation devices.
The goal is to restore normal tension—not too tight (which could limit motion), nor too loose (which could compromise stability).
5. Closure and Initial Immobilization
Once the graft is securely in place, the soft tissues are closed in layers. The arm is placed in a splint or brace in partial flexion to protect the repair during early healing.
Postoperative recovery is phased:
- Initial immobilization.
- Gradual range-of-motion exercises.
- Progressive strengthening.
- Sport-specific training and return to throwing.
Full return to competitive play may take 9 to 12 months for elite throwers.
6. Recent Innovations: Toward Personalized Surgery
Tommy John surgery continues to evolve with innovations such as:
- Minimally invasive techniques that reduce tissue disruption.
- Internal Brace augmentation, where a synthetic tape supports the graft for faster recovery in some cases.
- Patient-specific protocols, adjusting the graft type and surgical approach based on age, sport, and level of play.
The experience of the surgeon, the quality of the graft, and the athlete’s commitment to rehabilitation are all critical to long-term success.
Diagnosis and testing
Physical Exam
- Palpation:
- The healthcare professional palpates the elbow area looking for tenderness, swelling, or possible deformities.
- Mobility Assessment:
- Elbow movements, including flexion, extension, pronation, and supination, are assessed for limitations or unusual pain.
- Valgus and Varus Stress:
- Stress tests, such as the valgus test (to assess the UCL) and the varus test (to assess the radial collateral ligament), are performed to assess elbow stability.
Specialized Tests
- Rotator Cuff Test:
- Specific tests, such as the rotator cuff test, may be performed to rule out other possible causes of elbow pain.
Imaging Exams
- X-rays:
- Standard x-rays help rule out bone fractures and visualize the general structure of the elbow joint.
- Ultrasound:
- Ultrasound can be used to assess the real-time structure and movement of the ulnar collateral ligament.
- MRI (Magnetic Resonance Imaging):
- MRI provides detailed visualization of soft tissues and can detect tears, stretches or abnormalities in the ligament.
- Arthroscopy:
- In some cases, an arthroscopy may be performed, allowing direct visualization of the inside of the joint to confirm the diagnosis and make repairs if necessary.
The Osteopathic Approach in Post-Surgical Rehabilitation
Preparing, Supporting, and Reintegrating the Global Motion
UCL reconstruction surgery is a high-precision orthopedic act, but it is not the beginning—nor the end—of the healing journey. Around this surgical pivot lies a broader therapeutic process, where osteopathy plays a vital role—both before and after the intervention. Its objective: to optimize biomechanical balance, prevent compensations, and help the athlete reintegrate movement into a coherent, whole-body dynamic.
Preoperative Phase: Restoring Functional Biomechanics
Although surgery is often the inevitable outcome of a chronic ligament injury, osteopathic intervention before the operation can reduce excess strain, relieve compensatory overloads, and correct postural asymmetries that may have contributed to the lesion.
In the preoperative phase, osteopathic care may include:
- Postural realignment, focusing on the scapular-cervical-thoracic chain.
- Releasing diaphragm restrictions, which influence trunk rotation and breathing coordination—critical during throwing.
- Improving costal, vertebral, and scapular mobility to distribute forces more evenly.
- Identifying dysfunctional chains, whether descending (shoulder to elbow) or ascending (pelvis or feet to upper limb).
While this preparatory work won’t prevent surgery if a rupture is complete, it creates a healthier fascial and articular environment, making post-op recovery smoother and more integrated.
Postoperative Phase: Supporting Tissue and Functional Recovery
Even when technically perfect, surgery leaves traces—from fascial tension and proprioceptive changes to compensatory motor patterns. Osteopathic care complements physiotherapy by focusing on:
- Mobilizing scar tissue and surrounding fascia using gentle, precise techniques to restore elasticity and reduce adhesions.
- Releasing the diaphragm and thoracic area, often affected by immobilization or altered breathing patterns post-surgery.
- Balancing cervical and scapular tensions, frequently overloaded as part of protective or adaptive movement strategies.
- Preventing side dominance or asymmetrical compensation, especially when the non-dominant arm is overused during the recovery phase.
Timing is crucial: intervention must be neither too early (which risks disrupting healing), nor too late (which allows maladaptive patterns to set in). Collaboration with the physiotherapist and medical staff is essential, following a multidisciplinary and integrative approach.
Reintegrating the Throw: Beyond the Surgical Scar
Surgical success is not only measured by the strength of the graft, but by the athlete’s ability to recover fluid, powerful, and confident movement. During this re-training phase, osteopathy supports the process by:
- Reconnecting myofascial chains, including the deep front line, posterior spiral, and crossed functional lines.
- Restoring global proprioception, often diminished after weeks of immobilization and reduced athletic activity.
- Addressing emotional blocks and psychological apprehension, especially fear of re-injury or performance anxiety.
Because every injury also leaves a somatic imprint, athletes may unconsciously adapt their movement, protect the affected limb, or lose trust in their own bodies. Osteopathy offers a way to re-establish whole-body coherence, integrating not just structure and function, but sensation, rhythm, and awareness.
Injury Prevention in Throwing Sports: Strength, Rest, and Rhythm
The ligament shouldn’t have to break to get our attention
While Tommy John surgery has become a well-established solution for UCL injuries, prevention remains the most powerful—and often underutilized—tool in protecting the elbows of throwing athletes. The rising rates of UCL tears, particularly among adolescents, are not simply a consequence of bad luck. They are the outcome of excessive specialization, biomechanical overload, poor recovery habits, and training imbalances. Understanding how to prevent these injuries means shifting the focus from repair to preservation.
Respecting the Body’s Natural Limits
Throwing at high velocity is not a natural motion—it’s a biomechanical feat that places tremendous stress on the body, especially the elbow. The valgus torque during pitching can reach or even exceed the UCL’s natural tolerance. When athletes throw too frequently, too early in the season, or without adequate rest, this ligament has little chance to recover.
Key strategies to reduce risk include:
- Strict pitch counts and rest periods, particularly for youth and amateur athletes.
- Avoiding year-round single-sport specialization, which limits overall neuromuscular development and promotes repetitive stress.
- Limiting high-intensity throwing during growth spurts, when the bones and soft tissues are not yet fully adapted to withstand strain.
The concept of “throwing economy” should be promoted—emphasizing quality over volume, and form over intensity.
Strengthening the Entire Kinetic Chain
The elbow is not an isolated structure. It is a transfer point in a kinetic chain that begins at the feet and ends at the fingertips. Weaknesses or restrictions in one area often result in compensatory stress elsewhere—typically at the elbow.
A comprehensive prevention program should include:
- Scapular stabilization exercises, to optimize shoulder mechanics.
- Rotator cuff strengthening, to support deceleration and control during follow-through.
- Core strengthening, to improve trunk rotation and pelvic control.
- Hip mobility and strength, to generate force from the lower body and reduce stress on the upper limb.
In addition to isolated muscle training, athletes benefit from integrated movement drills that reproduce the rhythm and coordination of throwing—without the full force.
Mobility and Breathing: The Forgotten Players
Many prevention programs focus on strength and volume but overlook mobility and breathing—two essential pillars of throwing efficiency.
- Thoracic spine mobility is critical for trunk rotation. If restricted, the arm is forced to compensate, increasing elbow strain.
- Rib cage and diaphragm mobility support proper breathing patterns and trunk control during explosive movements.
- Breath holding during pitching (often unconscious) can create excessive upper body tension, destabilizing the scapular base.
Osteopathic assessment can help uncover these restrictions, often long before pain appears.
Load Management and Early Warning Signs
The concept of load management has gained traction in recent years, particularly in professional sports. Applied correctly, it involves balancing training intensity, volume, and recovery in a way that supports tissue adaptation without overuse.
Coaches, parents, and athletes should be trained to recognize early signs of strain:
- Decreased throwing velocity.
- Loss of control or accuracy.
- Medial elbow soreness after practice.
- A sense of “tightness” or “heaviness” in the arm.
These signs often precede structural damage—and offer a window for intervention before surgery becomes necessary.
The Role of Osteopathy in Prevention
Osteopaths can play a crucial role in prevention by identifying:
- Subtle asymmetries or restrictions in posture, mobility, and fascial tension.
- Breathing dysfunctions that affect coordination and endurance.
- Neuromuscular imbalances in the throwing chain.
By restoring global balance and improving the body’s adaptability, osteopathy helps reduce the cumulative strain that leads to ligament failure. It complements strength and conditioning by addressing the quality of movement, not just its quantity.
Cross-Disciplinary Perspectives: Surgery, Osteopathy, and Human Performance
Repairing the ligament is one thing—what about restoring movement, perception, and meaning?
UCL reconstruction surgery stands as a remarkable testament to the progress of sports medicine. It saves careers, restores lost function, and pushes the biological limits of the human body. But in celebrating technical success, are we at risk of reducing the athlete to a graft, a stabilized joint, or a return-to-play statistic? Biomedical precision, valuable though it is, cannot fully address the complex, lived reality of the injured athlete. This is where osteopathy enters—not to compete, but to complement, to rebalance, and to humanize the process of recovery.
Surgical Repair: A Mechanical Achievement
Tommy John surgery delivers impressive outcomes: over 85% of athletes return to their previous level, some even stronger than before. It’s a feat of modern orthopedic ingenuity and a testament to the body’s capacity to heal when given the proper structural foundation.
Yet this mechanical success has limitations:
- Recovery is long, demanding, and not always linear.
- Secondary issues may persist: stiffness, compensatory pain, altered movement.
- Surgery does not address the root biomechanical or postural imbalances that often contributed to the injury in the first place.
Put simply, reconstructing the ligament is not the same as restoring the movement that once defined the athlete.
Osteopathy: Reconnecting What Surgery Separates
Osteopathy does not seek to replace surgery, but rather to complete the picture—focusing on what isolated medical interventions cannot: the integration of movement, posture, emotion, and sensory feedback.
An osteopath asks different questions:
- How did this athlete’s body adapt and compensate before surgery?
- What hidden movement patterns or tensions remain after the ligament is repaired?
- Is their breath fluid? Is their trunk rotation symmetrical? Are they grounded when they throw?
- What does the body express in what it avoids, repeats, or alters without conscious awareness?
In this way, osteopathy helps reconnect mechanics with meaning, restoring not only function but embodied coherence.
Toward a More Conscious and Sustainable Performance
Elite sport pushes human limits—but it can also wear the body down. A holistic approach, such as osteopathy, supports:
- Early detection of dysfunctions, long before structural failure occurs.
- Release of chronic tension, before it crystallizes into pathology.
- Enhancement of proprioception and motor intelligence.
- Support for identity reconstruction, as athletes recover not just their skills but their sense of self.
Because true return-to-play isn’t just about clearance from a doctor—it’s about regaining trust in the body, the joy of movement, and the natural rhythm of performance.
The Body as a Therapeutic Dialogue
This cross-disciplinary view—surgery, rehabilitation, and osteopathy—is not about conflict. It’s about collaboration, where each practitioner brings their strengths, their timing, their perspective. The surgeon restores structure. The physiotherapist rebuilds strength and mobility. The osteopath reweaves the web of connection.
Together, they offer a global, integrated approach—one that respects the body’s logic, listens to its signals, and acknowledges the mind-body dimensions of recovery.
Conclusion: Beyond the Ligament—Listening to What the Body Tells Us
Tommy John surgery is a powerful symbol of what modern medicine can achieve: a tendon replaced, a career saved, a function restored. And yet, if we stop there—if we only see the success in terms of structure—we risk missing the deeper story written in the tissues.
The elbow is not just a joint. It is a crossing point of forces, intentions, and lived experience. The ligament doesn’t rupture by accident; it gives way after years of imbalance, tension, repetition, and perhaps silence. In this sense, the injury is not just mechanical—it is meaningful. It speaks. And the role of the therapist—whether surgeon, physiotherapist, or osteopath—is not only to repair, but to listen.
Osteopathy reminds us that true healing doesn’t happen in isolation. It emerges when the body is re-integrated into a whole, when function is restored within rhythm, when movement once again feels natural—not forced. The postoperative journey, then, becomes not just a return to sport, but an invitation: to move differently, to breathe more freely, to feel more fully, and to relate to one’s body with renewed attention.
In the end, the most important question may not be “Is the ligament stable?” but rather: “What has this injury revealed about the way I move, perform, and live?”
This is not a conclusion—it’s a transition. One that opens a space where high-level performance, deep somatic awareness, and interprofessional collaboration can truly meet.
References
Seidi, F., Rajabi, R., Ebrahimi, E., et al. (2014). The role of core stability in the prevention and rehabilitation of athletic injuries. Journal of Bodywork and Movement Therapies, 18(1), 152–157.
➤ Emphasizes kinetic chain and trunk stabilization in athletic health.
Ahmad, C. S., Grantham, W. J., & Greiwe, R. M. (2012). Public perceptions of Tommy John surgery. Physician and Sportsmedicine, 40(2), 64–72.
➤ Highlights misconceptions about the surgery improving performance rather than restoring function.
Erickson, B. J., et al. (2014). Performance and return to sport after Tommy John surgery among Major League Baseball pitchers. American Journal of Sports Medicine, 42(3), 536–543.
➤ Offers outcome data on return-to-play and performance levels post-surgery.
Cain, E. L., Dugas, J. R., Wolf, R. S., Andrews, J. R. (2010). Elbow injuries in throwing athletes: A current concepts review. American Journal of Sports Medicine, 38(7), 1367–1384.
➤ Comprehensive overview of UCL injuries and their treatment.
Paletta, G. A., & Wright, R. W. (2006). The modified docking technique for UCL reconstruction. Techniques in Shoulder and Elbow Surgery, 7(3), 145–153.
➤ Describes modern surgical approaches to UCL repair.
Petty, D. H., Andrews, J. R., Fleisig, G. S., Cain, E. L. (2004). Ulnar collateral ligament reconstruction in high school baseball players. American Journal of Sports Medicine, 32(5), 1158–1164.
➤ Early return-to-play statistics and surgical outcomes in young athletes.
Fleisig, G. S., & Andrews, J. R. (2012). Prevention of elbow injuries in youth baseball pitchers. Sports Health, 4(5), 419–424.
➤ Discusses injury mechanisms and practical preventive guidelines.
Wilk, K. E., Reinold, M. M., Dugas, J. R., et al. (2013). Current concepts in the rehabilitation of the overhead throwing athlete. American Journal of Sports Medicine, 41(2), 403–417.
➤ Evidence-based rehab protocols for post-Tommy John recovery.
Greenman, P. E. (2010). Principles of Manual Medicine (3rd ed.). Lippincott Williams & Wilkins.
➤ Foundational text linking somatic dysfunction with musculoskeletal imbalances—helpful for osteopathic context.
King, H. H., Tettambel, M. A., Lockwood, M. D., Johnson, K. H., Arsenault, D. A., Quist, R. (2003). Osteopathic manipulative treatment in sports medicine. Journal of the American Osteopathic Association, 103(12), 620–624.
➤ Review of how osteopathy supports athletes through recovery and injury prevention.















{kind=link}