
")
Introduction
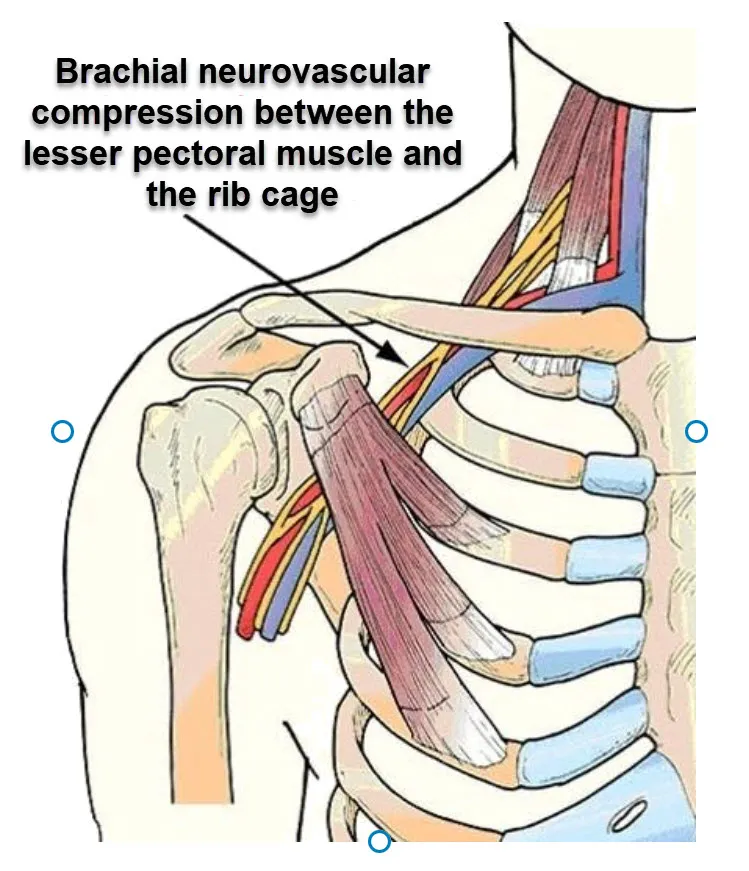
The pectoralis minor muscle is a lesser-known but vital muscle in the human body, situated in the chest region. Despite its small size compared to its counterpart, the pectoralis major, the pectoralis minor plays a significant role in shoulder movement and stability. However, when this muscle becomes tight or overactive, it can contribute to a condition known as Thoracic Outlet Syndrome (TOS), which can lead to a variety of symptoms and functional limitations.
To comprehend the role of the pectoralis minor in TOS, it’s crucial to first understand the anatomy of the region. The pectoralis minor originates from the third, fourth, and fifth ribs and inserts into the coracoid process of the scapula. This positioning allows it to influence the position of the shoulder complex and the surrounding neurovascular structures, such as the brachial plexus and the subclavian artery and vein, collectively referred to as the thoracic outlet.
In individuals with TOS, the pectoralis minor muscle often becomes shortened and tight due to poor posture, repetitive overhead activities, or even stress. This tightness can lead to compression of the neurovascular structures passing beneath it, causing symptoms such as pain, numbness, tingling, and weakness in the upper limb. Additionally, the compression of the subclavian artery may result in vascular symptoms, such as coldness or discoloration of the hand.
One common scenario contributing to TOS involves individuals who spend prolonged periods sitting at a desk or using computers, which can promote rounded shoulder posture and increased tension in the pectoralis minor. Over time, this can lead to a cascade of symptoms as the compressed structures struggle to function optimally.
Treatment for TOS often involves a multi-faceted approach, addressing both the muscular imbalances and the contributing factors. Physical therapy aimed at stretching and strengthening the pectoralis minor, along with other relevant muscles, can help alleviate symptoms by restoring balance and improving posture. Additionally, ergonomic modifications in the workplace and lifestyle changes may be necessary to prevent recurrence.
Anatomy of the Pectoralis Minor
The pectoralis minor, or serratus minor muscle (Pectoralis minor in English), is a muscle located in the anterior part of the rib cage. It lies deep to the pectoralis major and is attached to several bony structures, including the first three ribs.
- Origin: The small pectoral has its origin on the third, fourth and fifth ribs.
- Path: It goes upwards and inwards.
- Insertion: It attaches to the external blade of the scapula (scapula).
- Innervation: The muscle is innervated by the medial pectoral nerve.
Causes of Pectoralis Minor Syndrome
Pectoralis minor syndrome, also called pectoralis minor muscle tear syndrome, originates from compression or irritation of the lateral thoracic nerve (TLN) through the pectoralis minor muscle. Understanding the causes of this syndrome is essential to establish an effective treatment plan and relieve associated symptoms.
The main cause of pectoralis minor syndrome is compression of the lateral thoracic nerve as it passes through the pectoralis minor muscle. This compression can arise from a variety of factors, and one of the most common is increased muscle tension in the pectoralis minor. Excessive muscle contraction or spasm in this area can cause compression of the nerve, triggering the characteristic symptoms of the syndrome.
Another potential cause of pectoralis minor syndrome is the presence of trigger points in the muscle itself. Trigger points are hypersensitive areas in the muscle that can cause pain to radiate to other parts of the body when activated. In the case of the pectoralis minor, these trigger points can contribute to compression of the lateral thoracic nerve, exacerbating the symptoms of the syndrome.
Direct injuries to the pectoralis minor muscle may also play a role in the development of the syndrome. Trauma, such as a muscle tear or contusion, can cause anatomical changes in the muscle, creating a favorable environment for compression of the lateral thoracic nerve.
Repetitive activities or excessive movements of the arm above the head, constantly straining the pectoralis minor muscle, can contribute to the occurrence of the syndrome. Professionals exposed to repetitive motion, such as athletes or workers performing frequent manual tasks, may be more predisposed to developing this condition.
Finally, individual anatomical factors may also influence predisposition to pectoralis minor syndrome. Anatomical variations, such as the presence of an additional cervical rib, can create a more restricted space through which the lateral thoracic nerve passes, increasing the risk of compression.
- Muscle Hypertrophy or Tension: Hypertrophy or excessive tension of the pectoralis minor can result from a variety of situations, such as repetitive activities involving the arms, poorly executed shoulder movements, or heavy loads supported by the muscle.
- Poor Posture: Improper posture, particularly forward shoulder posture and forward lean, can contribute to overuse and strain of the pectoralis minor. This can be caused by daily habits, prolonged office work, or activities that constantly strain the muscles of the front part of the upper body.
- Injuries or Trauma: Direct injuries to the shoulder, neck or ribcage region can lead to muscular compensations, contributing to tension in the pectoralis minor. Accidents, falls or repeated trauma can be triggers.
- Muscular Imbalances: Imbalances between opposing muscles, such as the muscles of the front and back of the upper body, can put excessive strain on the pectoralis minor. People with relative back muscle weakness may be more likely to develop tightness in the pectoralis minor.
- Anatomical Abnormalities: Some individuals may have anatomical variations that promote compression at the thoracic outlet, thereby increasing the risk of developing pectoralis minor syndrome.
- Emotional Stress: Emotional stress can contribute to muscle tension throughout the body, including the pectoralis minor. High levels of stress can worsen symptoms and make it more difficult to manage the syndrome.
- Muscle tear: A tear or injury to the pectoralis minor can lead to inflammation and compression of the lateral thoracic nerve (TLN), contributing to the development of the syndrome.
- Repetitive movements: Certain activities or occupations that involve repetitive arm and shoulder movements, such as lifting heavy objects repeatedly, may increase the risk of developing this syndrome.
- Excessive muscle activity: Excessive muscle activity in the pectoralis minor region, for example from overuse or strenuous exercise, can cause irritation and compression of the nerve.
- Anatomical abnormalities: Anatomical variations, such as variations in the structure of the pectoralis minor or abnormalities in the way the lateral thoracic nerve passes through the muscle, may contribute to the syndrome.
- Traumatic Injuries: Traumatic injuries, such as bumps or chest injuries, can damage the pectoralis minor and lead to the development of symptoms.
- Nerve Compression: Nerve compression due to external factors such as tumors or pressure on the nerve can also contribute to pectoralis minor syndrome.
It is important to note that these causes can sometimes be interrelated, and there may be multiple factors contributing to the development of pectoralis minor syndrome in a given person.
Symptoms
Pectoralis minor syndrome, characterized by compression or irritation of the lateral thoracic nerve through the pectoralis minor muscle, presents with a range of identifiable symptoms. Understanding these symptoms is crucial for accurate diagnosis and effective management of this medical condition.
One of the most common symptoms of pectoralis minor syndrome is pain. Affected individuals may experience localized pain in the chest area, often described as a shooting or burning pain. This pain can extend to the upper arm, shoulder and sometimes the neck, following the trajectory of the lateral thoracic nerve.
The pain associated with this syndrome can be exacerbated by certain movements or activities. For example, raising the arm above the head, rotating movements, or holding a prolonged position can intensify the pain. This increased sensitivity to specific movements may help differentiate pectoralis minor syndrome from other conditions.
Another commonly observed symptom is the feeling of tingling or numbness in the affected area. These abnormal sensations, also known as paresthesias, may accompany pain and are often associated with the course of the affected lateral thoracic nerve.
Muscle weakness in the arm on the affected side may also be a symptom of pectoralis minor syndrome. Individuals may experience a decrease in muscle strength, which can affect their functional abilities in daily activities.
In addition to physical symptoms, the syndrome can also impact individuals’ emotional well-being. Persistent pain and functional limitations can lead to stress, anxiety, and sometimes depression. Holistic management of this condition should therefore take into account these psychosocial aspects.
It is essential to note that the symptoms of pectoralis minor syndrome can vary from person to person. Some individuals may experience a full range of symptoms, while others may only experience certain manifestations. An accurate diagnosis, based on a thorough clinical evaluation and sometimes additional tests such as electromyography (EMG) or nerve conduction studies, is crucial to guide the appropriate treatment plan.
- Pain: Pain is one of the most common symptoms. It may occur in the upper chest and radiate to the shoulder, arm or back of the affected side.
- Numbness or tingling: Some individuals may experience numbness or tingling sensations in the area innervated by the lateral thoracic nerve.
- Muscle weakness: Muscle weakness in the arm or hand on the affected side may occur.
- Increased sensitivity: The affected area may be more sensitive to touch, and unusual sensations may be felt.
- Loss of coordination: In some cases, loss of coordination in the affected arm may occur, which may affect the ability to perform precise movements.
- Muscle atrophy: Muscle atrophy (decrease in muscle size) may occur as the condition progresses, particularly if nerve compression persists.
- Discomfort during certain activities: Symptoms may be exacerbated during specific activities that strain the pectoralis minor muscle or lateral thoracic nerve.
Pathophysiology
The pathophysiology of pectoralis minor syndrome relies on compression of the lateral thoracic nerve (TLN) through the pectoralis minor muscle, resulting in a cascade of events that contribute to the observed symptoms. Understanding this pathological sequence is crucial to guide treatment approaches and improve the management of this condition.
It all starts with compression of the lateral thoracic nerve. This nerve, which runs through the pectoralis minor muscle, is susceptible to compression due to various factors, including muscle tension, postural imbalances, or even anatomical abnormalities. When the nerve is compressed, it can generate pain signals and sensory abnormalities, triggering the characteristic symptoms of the syndrome.
Compression of the nerve can also cause local inflammation. Inflammation is the body’s natural response to irritation or injury, and in the context of pectoralis minor syndrome, it contributes to pain and abnormal sensations. Inflammation can make compression worse by increasing pressure on the nerve, creating a vicious cycle of symptoms.
Muscle spasms of the pectoralis minor are another component of the pathophysiology of this syndrome. Excessive muscle tension, often in response to compression and inflammation, leads to muscle spasms. These spasms can not only worsen nerve compression but also change the biomechanics of the hip joint, contributing to symptoms.
As muscle spasms persist, they can lead to contractures of the pectoralis minor muscle. Muscle contractures are persistent and involuntary shortening of muscle fibers, limiting normal mobility of the joint. These contractures contribute to the modification of joint mechanics, introducing instability into the hip joint.
Joint instability results from changes in the shape and structure of the pectoralis minor muscle under the influence of muscle spasms and contractures. This instability, combined with pain, often prompts individuals to reduce the weight carried on the affected hip, thereby creating a reduction in weight carried.
Prolonged changes in joint mechanics, muscular imbalances and reduced weight carried can lead to secondary changes and deformities in the hip joint. These structural changes may contribute to the persistence of symptoms and chronicity of the syndrome.
- Anatomy of the Pectoralis Minor:
- The pectoralis minor muscle is located below the collarbone and attaches to the first rib. It is involved in the movement of the shoulder girdle and may also play a role in breathing.
- Vascular and Nervous Compression:
- A condition known as thoracic outlet syndrome can sometimes be associated with the pectoralis minor muscle. This syndrome may involve compression of the blood vessels (subclavian artery) or nerves (brachial plexus) that pass through the thoracic outlet region, located between the clavicle and the first rib.
- Triggering Symptoms:
- If the pectoralis minor muscle is hypertrophied, contracted or if there are anatomical abnormalities in the area, this can lead to compression of the structures mentioned above. This may trigger symptoms such as pain, numbness, weakness, or tingling in the arm, shoulder, or hand.
- Scapula Hyperabduction Syndrome:
- A less common condition but associated with the pectoralis minor muscle is scapula hyperabduction syndrome. It can manifest as a limitation of shoulder abduction due to abnormal contraction of the muscle.
- Trauma or Injury:
- Trauma or injury to the clavicle or first rib can also affect the pectoralis minor muscle and contribute to symptoms.
- Diagnosis and Treatment:
- Diagnosis of conditions associated with the pectoralis minor muscle generally relies on clinical assessment, medical imaging (such as X-rays, MRIs, or ultrasounds), and tests of nerve or vascular function. Treatment may include physical therapy, pain management, and in some cases, surgical procedures to release compressed structures.
Diagnosis of Pectoralis Minor Syndrome
Diagnosing pectoralis minor syndrome (PMS) involves a comprehensive approach combining clinical assessment, imaging, and specialized tests to identify the compression or irritation of neurovascular structures beneath the pectoralis minor muscle. Accurate diagnosis is crucial to distinguish PMS from other conditions, such as thoracic outlet syndrome or cervical spine disorders, which can present with similar symptoms.
Clinical Assessment
A detailed clinical evaluation forms the foundation of diagnosis. The process includes:
- Patient History:
- Patients typically report pain in the chest, shoulder, or arm, along with symptoms such as numbness, tingling, or weakness. These symptoms may worsen with prolonged use of the arm in elevated positions or repetitive overhead activities.
- A history of poor posture, repetitive motion, or trauma to the chest or shoulder can provide critical diagnostic clues.
- Physical Examination:
- Postural Assessment: A forward shoulder posture or rounded upper back may indicate tension or shortening of the pectoralis minor muscle.
- Palpation: Tenderness or tightness in the pectoralis minor region, particularly near the coracoid process, can suggest muscle involvement.
- Range of Motion Tests: Restricted scapular mobility or discomfort during specific shoulder movements may indicate muscle dysfunction.
- Neurological and Vascular Symptoms: Clinical tests may assess for diminished pulses, changes in hand coloration, or sensory deficits indicative of neurovascular compression.
Imaging
Imaging studies support clinical findings and help exclude other potential causes of symptoms:
- X-rays:
- Used to detect bony abnormalities, such as cervical ribs, that may contribute to thoracic outlet compression.
- Ultrasound:
- Identifies soft tissue abnormalities, such as hypertrophy of the pectoralis minor or impingement of neurovascular structures.
- Magnetic Resonance Imaging (MRI):
- Offers detailed visualization of the pectoralis minor, surrounding muscles, and adjacent neurovascular structures. It helps identify structural changes or inflammation.
- Computed Tomography (CT):
- Occasionally used to provide cross-sectional imaging of the thoracic outlet for more complex cases.
Special Tests
Special tests help confirm the involvement of the pectoralis minor muscle in symptom generation. Among these, the Wright test is a widely used and effective diagnostic maneuver:
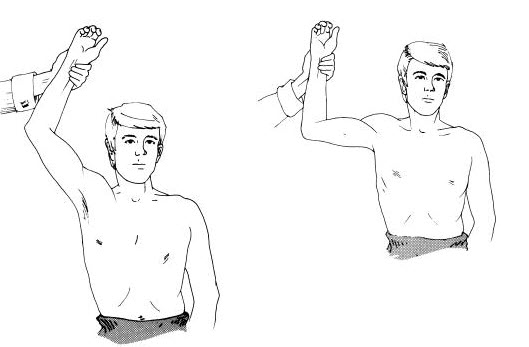
- Wright Test (Hyperabduction Test):
- The patient’s arm is brought overhead in the coronal plane, hyperabducting the shoulder while maintaining the elbow extended.
- During this maneuver, the clinician palpates the radial pulse on the test arm.
- A positive test is indicated by:
- A significant reduction or absence of the radial pulse.
- Reproduction of the patient’s symptoms, such as pain, numbness, or tingling.
- The test helps confirm compression of the neurovascular structures under the pectoralis minor muscle during shoulder movement.
- Adson’s Test:
- Although primarily for thoracic outlet syndrome, it can help identify neurovascular compression due to pectoralis minor involvement by assessing changes in pulse or symptoms with neck rotation and shoulder abduction.
- Palpatory Compression Test:
- Direct pressure is applied to the pectoralis minor region to reproduce symptoms, providing a more localized diagnostic indication of PMS.
Osteopathic Treatment Approaches
Osteopathic treatment of pectoralis minor syndrome aims to relieve compression or irritation of the lateral thoracic nerve through the pectoralis minor muscle. Osteopathy takes a holistic approach, seeking to restore muscular balance, improve mobility of affected structures and alleviate associated symptoms. Here are some techniques commonly used in the osteopathic treatment of this condition:
- Myofascial Release: This technique aims to release tension in the connective tissue surrounding the muscles, known as fascia. The osteopath uses slow, gentle movements to stretch and release the fascia of the pectoralis minor, thus promoting better mobility.
- Gentle Manipulations: Gentle joint manipulations are used to restore mobility to the joints of the rib cage. This may include specific movements for the ribs, scapula, and other joints associated with the pectoralis minor.
- Targeted Stretches: Specific stretching exercises may be recommended to stretch the pectoralis minor and improve its flexibility. These stretches can be adapted to the patient’s individual condition and are often integrated into a rehabilitation program.
- Trigger Point Management: Trigger points are areas of tension located in the muscles. The osteopath can apply targeted pressure to these points to release tension and relieve associated pain.
- Muscle Strengthening Exercises: To restore muscular balance, strengthening exercises may be prescribed, with emphasis on the antagonist muscles of the back to counter excessive tension in the pectoralis minor.
- Education and Advice: The osteopath will provide advice on posture, changes in daily habits and self-care techniques to help the patient prevent the recurrence of tightness in the pectoralis minor.
- Relaxation Techniques: Stress can contribute to muscle tension. The osteopath can teach relaxation techniques, such as deep breathing, to help reduce stress and associated tension.
- Monitoring and Adjustments: The treatment plan is generally tailored to the patient’s individual response. Follow-up sessions may be recommended to monitor progress and make adjustments to treatment if necessary.
Evidence-Based Osteopathic Interventions for Thoracic Outlet Syndrome with Pectoralis Minor Involvement
1. “New Proposal of Evaluation of the Thoracic Outlet” (2018)
- Authors: B. Bruno, M. Fabiola, M. Bruno, S. Beatrice
- Summary: This study reviews innovative evaluation and treatment methods for TOS focusing on pectoralis minor syndrome. Osteopathic palpation techniques effectively address thoracic outlet compression.
- Link: Read Article
2. “Thoracic Outlet Syndrome of Pectoralis Minor Etiology Mimicking Cardiac Symptoms on Activity: A Case Report” (2012)
- Author: G. Fitzgerald
- Summary: Case report showcasing osteopathic techniques targeting pectoralis minor compression, alleviating TOS symptoms misinterpreted as cardiac. Treatment highlighted postural corrections and myofascial release.
- Link: Read Article
3. “Exercise Rehabilitation for Neurogenic Thoracic Outlet Syndrome: A Scoping Review” (2022)
- Authors: D. Luu, R. Seto, K. Deoraj
- Summary: The review examines rehabilitation protocols, including osteopathic approaches, emphasizing pectoralis minor release and posture optimization for neurogenic TOS management.
- Link: Read Article
4. “A Case of Venous Thoracic Outlet Syndrome: Osteopathic Manipulative Technique Considerations” (2019)
- Authors: E. Yuschak, F. Haq, S. Chase
- Summary: This study integrates osteopathic techniques for venous TOS caused by pectoralis minor entrapment, emphasizing manual therapy and motion corrections.
- Link: Read Article
5. “Thoracic Outlet Syndrome: A Review for Primary Care Providers” (2021)
- Authors: R. Chipman, V. Onyeukwu
- Summary: Comprehensive review on TOS pathophysiology and management, emphasizing the role of osteopathy in addressing pectoralis minor compression.
- Link: Read Article
6. “An Osteopathic Approach to Conservative Management of Thoracic Outlet Syndromes” (1989)
- Author: R. Dobrusin
- Summary: This foundational study explores osteopathic methods, including myofascial release and joint mobilizations, targeting thoracic outlet and pectoralis minor tension.
- Link: Read PDF
7. “Thoracic Outlet Syndrome—Postural Type: Ultrasound Imaging of Pectoralis Minor and Brachial Plexus Abnormalities” (2012)
- Author: B.M. Sucher
- Summary: Demonstrates the role of imaging in diagnosing TOS and guides osteopathic treatment targeting the pectoralis minor’s role in compressing brachial plexus structures.
- Link: Read Article
8. “Therapist Management of Thoracic Outlet Syndrome” (1994)
- Author: M.T. Walsh
- Summary: Explores combined therapeutic approaches, including osteopathic manipulative therapy, for managing neurovascular compression in the pectoralis minor region.
- Link: Read Article
9. “Thoracic Outlet Syndrome Part 1: Clinical Manifestations, Differentiation and Treatment Pathways” (2010)
- Authors: L.A. Watson, T. Pizzari
- Summary: Discusses clinical differentiation of TOS types, emphasizing osteopathic interventions in pectoralis minor syndrome for improving symptoms and functionality.
- Link: Read Article
10. “Thoracic Outlet Syndrome Part 2: Conservative Management of Thoracic Outlet” (2010)
- Authors: L.A. Watson, S. Balster
- Summary: Focuses on conservative management strategies, highlighting osteopathy’s role in addressing pectoralis minor tightness and associated neurovascular issues.
- Link: Read PDF
Exercises and Rehabilitation for the Minor Pectoral
Minor Pectoral Stretches
- Wall corner stretch:
- Stand near a corner of the wall.
- Bend your elbow 90 degrees and place your forearm against the wall.
- Take a step forward with the foot on the side of the extended arm.
- Turn your body slightly to feel the stretch in the pectoralis minor.
- Hold the position for 30 seconds to 1 minute.
- Seated stretch:
- Sit on the floor with your legs crossed.
- Place your hands behind you, fingers pointing backwards.
- Move your hands back, lifting your shoulders away from the floor to stretch the pectoralis minor.
- Hold the position for 30 seconds to 1 minute.
Strengthening the Small Pectoral
- Tight elbows with elastic band:
- Attach an elastic band to a handle or fixed point at shoulder height.
- Hold the other end of the band with your opposite hand.
- Bend your elbow 90 degrees.
- Squeeze your elbows together, resisting the tension of the band.
- Perform 2 to 3 sets of 12 to 15 repetitions.
- Scapular elevations:
- Lie on your stomach on an incline bench with light dumbbells.
- Let the dumbbells hang toward the floor.
- Raise your shoulder blades toward the ceiling by contracting your pectoralis minor.
- Go back down slowly.
- Perform 2 to 3 sets of 12 to 15 repetitions.
Stabilization Exercises
- Side plank with rotation:
- Assume the one-arm side plank position.
- Turn your upper body toward the ceiling, opening your chest.
- Return to the starting position.
- Perform 2 to 3 sets of 10 repetitions on each side.
- Bridge with rotation:
- Lie on your back with your knees bent.
- Lift hips toward the ceiling to form a straight line from shoulders to knees.
- Turn your upper body to the left, then to the right, alternately.
- Perform 2 to 3 sets of 10 rotations on each side.
Prevention Tips
- Maintaining Good Posture:
- Ergonomics at work:
- Adjust the height of your chair and desk to maintain a neutral sitting position.
- Use an office chair that provides good lumbar support.
- Place your computer screen at eye level to avoid constantly lowering your head.
- Regular stretching:
- Take breaks every hour to stretch and change positions.
- Do neck, shoulder and back stretches to avoid excess tension.
- Ergonomics at work:
- Balanced Muscle Strengthening:
- Overall strengthening exercises:
- Incorporate strengthening exercises for the entire body, including the back muscles, to maintain muscular balance.
- Consult a fitness professional to develop a program tailored to your needs.
- Strengthening the small pectoral:
- Include specific pectoralis minor strengthening exercises, like those mentioned previously, in your workout routine.
- Overall strengthening exercises:
- Muscle Relaxation Techniques:
- Deep breathing :
- Practice deep breathing to relax your chest muscles.
- Inhale deeply through your nose, hold your breath for a few seconds, then exhale slowly through your mouth.
- Yoga and stretching:
- Yoga can be beneficial for improving flexibility and reducing muscle tension.
- Specific postures, such as downward dog and child’s pose, can help stretch the pectoralis minor.
- Deep breathing :
- Stress management :
- Stress management practices:
- Identify stressors and adopt stress management techniques, such as meditation, mindfulness, or engaging in relaxing hobbies.
- Active pause:
- Take active breaks during the day to move and release accumulated tension.
- Stress management practices:
- Medical consultation :
- If you experience persistent pain, consult a health professional, such as a physiotherapist, to assess your situation and provide you with advice tailored to your condition.
References
- Sanders RJ, Annest SJ. Thoracic outlet and pectoralis minor syndromes. Semin Vasc Surg. 2014;27:86–117. [ PubMed ] [ Google Scholar ]
- Sanders RJ, Rao NM. The forgotten pectoralis minor syndrome: 100 operations for pectoralis minor syndrome alone or accompanied by neurogenic thoracic outlet syndrome. Ann Vasc Surg. 2010;24:701–708. [ PubMed ] [ Google Scholar ]
- Elsayed HH, Soliman S, Hamed AM, El-Saqqa A, Hussein AT, BinMelhi E, et al. Venous pectoralis minor syndrome: A rare subdivision of the thoracic outlet syndrome. Interact Cardiovasc Thorac Surg. 2020;30:33–35. [ PubMed ] [ Google Scholar ]
- Aktaş İ, Kaya E, Akpınar P, Ünlü Özkan F, Vural A, Akgün K. Vascular pectoralis minor syndrome as an overlooked condition: A case report. Turk J Phys Med Rehabil. 2021;67:538–541. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Ramcharitar RK, Elghawy O, Man L, Sharma AM, Peruri A, Park AW, et al. Images in vascular medicine pectoralis minor syndrome – A forgotten vascular compression syndrome. Vasc Med. 2022;27:518–520. [ PubMed ] [ Google Scholar ]
- Sanders RJ, Rao NM. Pectoralis minor obstruction of the axillary vein: Report of six patients. J Vasc Surg. 2007;45:1206–1211. [ PubMed ] [ Google Scholar ]
- Illig KA, Rodriguez-Zoppi E, Bland T, Muftah M, Jospitre E. The incidence of thoracic outlet syndrome. Ann Vasc Surg. 2021;70:263–272. [ PubMed ] [ Google Scholar ]
- Hussain MA, Aljabri B, Al-Omran M. Vascular thoracic outlet syndrome. Semin Thorac Cardiovasc Surg. 2016;28:151–157. [ PubMed ] [ Google Scholar ]
- Vemuri C, Wittenberg AM, Caputo FJ, Earley JA, Driskill MR, Rastogi R, et al. Early effectiveness of isolated pectoralis minor tenotomy in selected patients with neurogenic thoracic outlet syndrome. J Vasc Surg. 2013;57:1345–1352. [ PubMed ] [ Google Scholar ]
- Hong CZ, Simons DG. Response to treatment for pectoralis minor myofascial pain syndrome after whiplash. J Musculoskelet Pain. 1993;1:89–132. [ Google Scholar ]
- Sucher BM. Thoracic outlet syndrome–a myofascial variant: Part 2. Treatment. J Am Osteopath Assoc. 1990;90:810–812. [ PubMed ] [ Google Scholar ]
- Lawson GE, Hung LY, Ko GD, Laframboise MA. A case of pseudo-angina pectoris from a pectoralis minor trigger point caused by cross-country skiing. J Chiropr Med. 2011;10:173–178. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Zajac JM, Angeline ME, Bohon TM, Loftus M, Potter HG, Weiland AJ, et al. Axillary artery thrombosis in a major league baseball pitcher: A case report and rehabilitation guide. Sports Health. 2013;5:402–406. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Moore MK. Upper crossed syndrome and its relationship to cervicogenic headache. J Manipulative Physiol Ther. 2004;27:414–420. [ PubMed ] [ Google Scholar ]
- Aktas I, Kaya E, Akpinar P, Atici A, Unlu Ozkan F, Palamar D, et al. Spasticity-induced pectoralis minor syndrome: A case-report. Top Stroke Rehab. 2020;27:316–319. [ PubMed ] [ Google Scholar ]
- Palamar D, Aktaş İ, Akgün K. Pectoralis minor syndrome miscible with subacromial impingement syndrome. South Clin Ist Euras. 2017;28:181–183. [ Google Scholar ]
- Kuhn JE, Lebus V GF, Bible JE. Thoracic outlet syndrome. J Am Acad Orthop Surg. 2015;23:222–232. [ PubMed ] [ Google Scholar ]
- Sanders RJ, Annest SJ, Goldson E. Neurogenic thoracic outlet and pectoralis minor syndromes in children. Vasc Endovascular Surg. 2013;47:335–341. [ PubMed ] [ Google Scholar ]
- Godfrey NF, Halter DG, Minna DA, Weiss M, Lorber A. Thoracic outlet syndrome mimicking angina pectoris with elevated creatine phosphokinase values. Chest. 1983;83:461–463. [ PubMed ] [ Google Scholar ]
- Fitzgerald G. Thoracic outlet syndrome of pectoralis minor etiology mimicking cardiac symptoms on activity: A case report. J Can Chiropractic Assoc. 2012;56:311–315. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Sanders RJ, Annest SJ. Pectoralis minor syndrome: Subclavicular brachial plexus compression. Diagnostics (Basel) 2017;7:46–46. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Caliş M, Akgün K, Birtane M, Karacan I, Caliş H, Tüzün F. Diagnostic values of clinical diagnostic tests in subacromial impingement syndrome. Ann Rheum Dis. 2000;59:44–47. [ PMC free article ] [ PubMed ] [ Google Scholar ]
- Neer CS 2nd. Impingement lesions. Clin Orthop Relat Res. 1983;173:70–77. [ PubMed ] [ Google Scholar ]
- Morais N, Cruz J. The pectoralis minor muscle and shoulder movement-related impairments and pain: Rationale, assessment and management. Phys Ther Sport. 2016;17:1–13. [ PubMed ] [ Google Scholar ]
- Rayan GM, Jensen C. Thoracic outlet syndrome: Provocative examination maneuvers in a typical population. J Shoulder Elbow Surg. 1995;4:113–117. [ PubMed ] [ Google Scholar ]
- Kleinrensink GJ, Stoeckart R, Mulder PG, Hoek G, Broek T, Vleeming A, et al. Upper limb tension tests as tools in the diagnosis of nerve and plexus lesions. Anatomical and biomechanical aspects. Clin Biomech (Bristol, Avon) 2000;15:9–14. [ PubMed ] [ Google Scholar ]
- Cruz-Martínez A, Arpa J. Electrophysiological assessment in neurogenic thoracic outlet syndrome. Electromyogr Clin Neurophysiol. 2001;41:253–256. [ PubMed ] [ Google Scholar ]
- Illig KA, Donahue D, Duncan A, Freischlag J, Gelabert H, Johansen K, et al. Reporting standards of the Society for Vascular Surgery for thoracic outlet syndrome. e23-35 J Vasc Surg. 2016;64 [ PubMed ] [ Google Scholar ]

















{kind=link}